Corresponding author: Asmita Priyadarshini Khatiwada, asmitapriyadarshinikhatiwada@gmail.com
DOI: 10.31662/jmaj.2020-0120
Received: December 24, 2020
Accepted: February 12, 2021
Advance Publication: April 2, 2021
Published: April 15, 2021
Cite this article as:
Giri A, Sapkota B, Shrestha R, Khatiwada AP, Tiwari R, Aryal M, Timilsina M, Bhujel B, Adhikari M, Sah R, Bhandari D, Ozaki A, Martellucci CA, Kotera Y, Mousavi SH, Shrestha S. A Narrative Review of Personal Protective Equipment Uses in Coronavirus Disease 2019 and Its Disposable Practices. JMA J. 2021;4(2):86-90.
Since severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), responsible for causing coronavirus disease 2019 (COVID-19), is transmitted through close contact and droplets, people, especially those at risk of infection, must follow preventive measures in the community and healthcare settings. Healthcare personnel (HCP) must appropriately select and use personal protective equipment (PPE) with sensible donning and doffing and disposal practices. A narrative review of the existing literature was conducted, in which articles from Scopus, PubMed, Google Scholar, ScienceDirect, and Web of Science were collected. The primary findings of the retained articles were reviewed according to official recommendations on PPE use. The World Health Organization (WHO), US Centers for Disease Control and Prevention (CDC), and European Center for Disease Control and Prevention (ECDC) recommend standard precautions for contact transmission, respiratory transmission, and droplet precautions among HCPs caring for patients with COVID-19. Indeed, healthcare workers working in high-risk areas, as well as the public, when social distancing cannot be assured, must wear PPE such as face mask and protective eyewear to prevent the transmission of SARS-CoV-2 infection. Due to the increased use of PPE, the potentially infectious waste stream has been rapidly increasing, requiring safe and adequate solid waste management. The proper use of PPE and management of waste generated from COVID-19 care centers can reduce the risk of COVID-19 infection. These measures should be implemented to counter the rapid spread and any long-term impacts of the current pandemic.
Key words: coronavirus disease 2019 (COVID-19), healthcare waste (HCW) management, personal protective equipment (PPE), severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
The first human case of coronavirus disease 2019 (COVID-19) caused by a novel coronavirus (severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was reported in Wuhan, China, in early December 2019. Coronaviruses have been responsible for several outbreaks, including the severe acute respiratory syndrome (SARS) pandemic of 2002-2003 and the Middle East respiratory syndrome outbreak of 2012, which originated in Saudi Arabia (1). A total of 101,406,059 COVID-19 cases and 2,191,898 deaths (as of January 30, 2021) around the world is reported by the World Health Organization (WHO) (2). While 81% of patients with COVID-19 have no symptoms or mild pneumonia, severe presentations, such as acute respiratory distress syndrome, occurs in 14% of patients (3), (4). Further, only 5% of patients present with respiratory failure, septic shock, and/or multiple-organ failure (4).
The human-to-human transmission of SARS-CoV-2 primarily occurs through direct, indirect, or close contact with infected people via respiratory secretions and saliva, or through their respiratory droplets, expelled when an infected person coughs, sneezes, talks, or sings (5), (6). Airborne transmission can also occur, although less frequently (7). As COVID-19 is primarily transmitted through close contact and droplets, those coming in contact with the infected or those at risk of infection must follow preventive measures in community and healthcare settings. Effective preventive measures in the community include maintaining hand and respiratory hygiene; avoiding touching one’s eyes, nose, and mouth; wearing a face mask; and maintaining at least two-meter distance from others, especially those who exhibit symptoms. In addition, healthcare workers must appropriately use personal protective equipment (PPE) (selecting the right PPE with proper donning and doffing and disposal of the used ones) when coming in contact with suspected or confirmed cases of COVID-19 (8). Therefore, this study aims to discuss the use of PPE and its disposal practices during the COVID-19 pandemic.
The present review focuses on the use of PPE as recommended by guidelines and its disposal practice after contact with suspected or active COVID-19 case. The databases of Scopus, PubMed, Google Scholar, ScienceDirect, and Web of Science were searched using the following search keywords: “COVID-19” OR “Personnel Protective Equipment” OR “PPE” OR “Disposal Practice” OR “PPE Disposal Practice” OR “PPE Guidelines” OR “Hospital waste.” The PPE use guidelines published by the WHO, US Centers for Disease Control and Prevention (CDC), and European Center for Disease Control and Prevention (ECDC) were included in this review. The PPE use guidelines of organizations beside those mentioned above were excluded. Articles containing original data on PPE use practices on community, hospital, and COVID-19 care center and articles on healthcare waste (HCW) disposal and management practices on community and hospital setting in context of COVID-19 were included in the review. Furthermore, PPE use and disposal of general practices were excluded. Articles published in the English language were included. The articles were selected based on relevance to COVID-19 and PPE use and disposal practice. Articles published from December 1, 2019, to October 5, 2020, were included for analysis purpose.
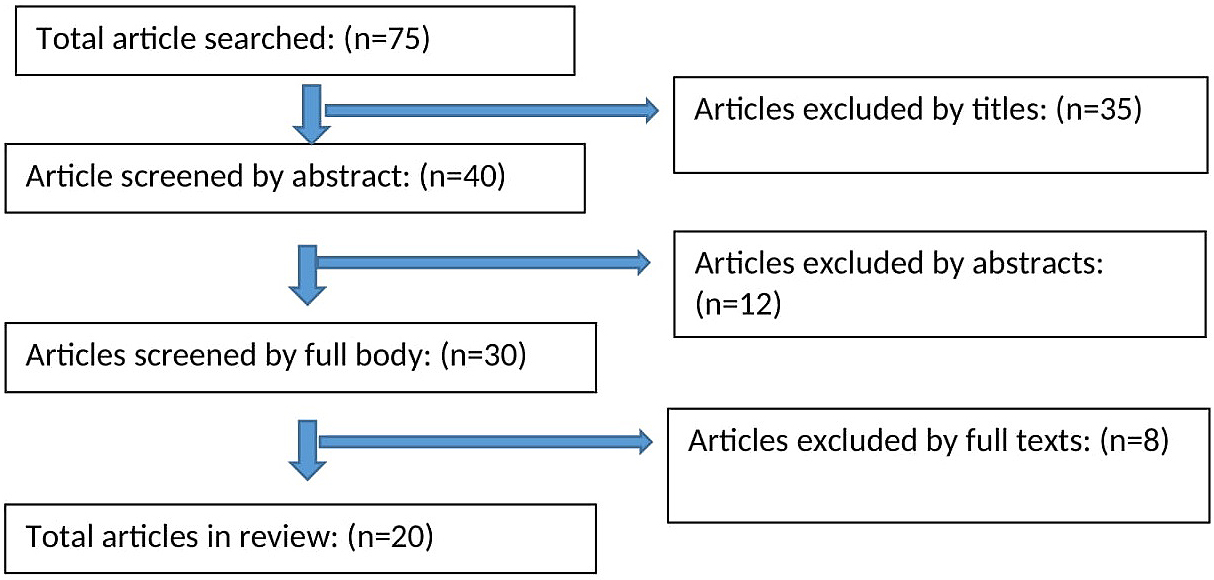
Table 1 shows comparison of PPE guideline recommendations by the WHO, CDC, and ECDC. Precautions against COVID-19 recommended by the WHO, CDC, and ECDC were summarized. A total of 75 articles were initially identified and 20 full texts were screened to verify inclusion and exclusion criteria, and 5 articles were retained for final review (Figure 1).
Table 1. Comparison of Personal Protective Equipment (PPE) Guideline Recommendations by the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and European Center for Disease Control and Prevention (ECDC).
| Setting/time issued | WHO (March 2020) | CDC (May 2020) | ECDC (March 2020) |
|---|---|---|---|
| Contact and droplet precautions | Medical mask | N95 or higher-level respirator | FFP2 or FFP3 respirator |
| Eye protection (goggles) or facial protection (face shield) | Eye protection (e.g., goggles, face shield) | Eye protection | |
| Clean, nonsterile, long-sleeved gown, gloves, and boots | Gloves | Gloves | |
| Isolation gown | Long-sleeved, water-resistant gown | ||
| Airborne precautions for aerosol-generating procedures | NIOSH-certified N95 | ||
| EU standard FFP2 /FFP3 or equivalent | |||
| Eye protection (i.e., goggles or a face shield) | N95 or higher-level respirator | FFP3 respirator | |
| Clean, nonsterile, long-sleeved gown | Eye protection | Eye protection | |
| Gloves | Gown | ||
| Waterproof apron (if gowns are not fluid-resistant) | Gloves | Gloves | |
| Collecting specimens (aerosol-generating procedures not included) | Medical mask | N95 respirator (or higher-level respirator) or face-mask (if a respirator is not available) | Surgical mask (if available, FFP2 respirator) |
| Eye protection | Eye protection | Eye protection | |
| Gown | Gown | Gown | |
| Gloves | Gloves | Gloves | |
| Drive-through or outdoor facilities | |||
| Surgical mask (in addition to gloves, goggles, and gown) | |||
| Inpatient care | Medical mask | N95 respirator (or higher-level respirator) or face-mask (if a respirator is not available) | FFP2 respirator |
| Eye protection | Eye protection | Goggles or face shield | |
| Gloves | Gown | Gown or apron | |
| Gown | Gloves | Gloves |
The PPE use practices and outcomes are listed in Table 2. The WHO recommends implementing droplet and contact precautions during nonaerosol-generating procedures of patients with COVID-19. Medical masks (surgical masks) and eye protection are recommended during direct care of patients to prevent droplet transmission. For contact precaution, long-sleeved, water-resistant gowns and gloves are recommended. Respirators such as N95 or filtering facepiece (FFP3) (standard or equivalent), gowns (aprons should be used if gowns are not fluid-resistant), gloves, eye protection, and aprons are recommended during aerosol-generating procedures on patients with COVID-19 (such as intubation, cardiopulmonary resuscitation, nebulization, and chest physiotherapy) (8). The CDC and ECDC recommend standard precautions for contact transmission, respiratory transmission, and droplet precautions among healthcare workers who look after patients with COVID-19 (9), (10). The WHO, CDC, and ECDC recommend rational use of PPE for healthcare personnel (HCP) when taking care of suspected patients with SARS-CoV-2 (8), (9), (10).
Table 2. Personal Protective Equipment (PPE) Use Practices and Outcomes.
| Authors | Country | Findings/outcomes and comments |
|---|---|---|
| Kumar J (19) | Pakistan | Health workers had a positive attitude but had moderate-to-poor level of knowledge and practice regarding face masks. Health workers and general public awareness campaigns regarding the proper use of face mask using all social media available resources would help this pandemic. |
| Lyu W (20) | USA | In the USA, states mandating face masks in public produced a more significant decline in daily COVID-19 growth rates than states that did not issue such mandates. |
| Liu M (21) | China | Frontline healthcare workers, provided with appropriate PPE for delivering health care to patients with COVID-19 (including aerosol-generating procedures) were found negative for SARS-CoV-2 nucleic acids and specific IgM and IgG antibodies. |
| Renaud PP (22) | Canada | The knowledge and practice regarding PPE use among healthcare workers were found to be inadequate and improper. Only 50% identified the correct donning and 35% correct doffing. The majority (70%) identified the need to perform hand hygiene before removing face mask and/or eye protection. |
| Ong JJY (23) | Singapore | The frequency of PPE use for healthcare workers increased during the COVID-19 emergency. The mostly used PPEs were N95 masks for respiratory system protection and goggles for eye protection. The majority of healthcare workers (81%) experienced PPE-associated headaches. The onset of headache was less than 60 min after donning the PPE and resolved within 30 min of PPE doffing. |
Additionally, all staff within the hospital must adopt hand hygiene, environmental disinfection, and proper waste management. Workers who are not involved in any COVID-19-relevant activity need not use PPE but should strictly follow standard precautions, such as maintaining a minimum distance of 2 meters between individuals, among others (8), (9), (10).
In addition to the provision of PPE, one must also concentrate on their proper use, especially appropriate donning and doffing procedures to minimize biosafety breaches and potential exposure to HCP (11).
The overall waste generated was reduced due to lockdown implemented in several nations, but the HCW generated increased due to single-use PPE. Among the total waste, PPE, gloves, tissue papers, face masks, and boots accounted for 10.8%, 1.7%, 10.0%, 1.6%, and 12.2%, respectively (12). Traditionally, PPE was predominantly used in the hospital environment, but because of the COVID-19 pandemic, PPE is widely used in community and household settings as well. Owing to the increased use of PPE, the potentially infectious waste in domestic solid waste streams has risen, urgently necessitating safe and adequate management of solid waste (13).
The WHO (July 29, 2020) published a guideline on water, sanitation, hygiene, and waste management for SARS-CoV-2, which included measures to be taken while managing HCW. HCWs generated from COVID-19 care centers are not different from other HCWs, and no additional waste management recommendation is needed (12). Nevertheless, the provision of safe water, sanitation, waste management, and hygiene conditions is required for infection prevention from HCWs. Potential infectious wastes, such as sharps, bandages, and pathological waste, must be safely collected and segregated, treated on-site, and then disposed of. Reusable PPE, such as utility gloves, heavy-duty gloves, and reusable plastic aprons, are cleaned with soap and water and then decontaminated with 0.5% sodium hypochlorite solution each time they are used, whereas single-use gloves and gowns must be discarded as infectious waste after each use (12).
In the developing country of Nepal, the Ministry of Health and Population published a guideline for HCW management in 2014 and COVID-related waste management in 2020. This guideline for disinfection delineates that reusable PPE must be washed with soap/detergent then autoclaved or soaked in 0.5% sodium hypochlorite solution for at least 30 minutes and finally washed with at least 10 times of the volume of clean water and dried before reuse. The guideline states that nonreusable PPE must be autoclaved or soaked in 0.5% sodium hypochlorite solution for 30 minutes and disposed of in a municipal landfill or burial pit (14).
During the COVID-19 outbreak in China, the disposal practice of HCPs has changed from the conventional technique to alternative techniques, such as from decentralization to centralization, from irregular to regular management, and from mostly incineration to non-incineration disposal technologies, such as steam (autoclave), dry heat, microwave sterilization, or chemical disinfection (15).
Disposable medical masks can be reused (during a shortage of masks) following disinfection with hydrogen peroxide vapor, ultraviolet or gamma irradiation, and ethylene oxide treatment (16). In many developing countries, specific techniques for the HCW management are absent. Thus, such waste is often disposed of alongside municipal solid wastes in the open or poorly managed landfills. Improper management of PPE while treating patients with COVID-19, such as using inadequate PPE or reusing them, has been shown to pose a significant risk for transmission (16), (17).
There are also instances of discarding single-use PPE, such as face masks and gloves, haphazardly in parking lots at the grocery stores, streets, and gardens. Such careless practice could increase the risk of transmission through waste materials and harm the environment since most of the PPE is made from nondegradable materials (18).
COVID-19 is a pandemic that has taken lives of more than 2 million people all over the world as of January 2021. HCPs, especially those working in high-risk areas, and those looking after patients with COVID-19 must use all required PPE, and the public, when physical distancing is impossible, must wear PPE, such as face masks, to prevent possible transmission of SARS-CoV-2 infection. Taken together with the recommendations from the literature, it is concluded that the proper use of PPE and proper management of HCWs generated from COVID-19 care centers can reduce the risk of COVID-19 spread.
Akihiko Ozaki received personal fees from MNES Inc., outside the submitted work.
All authors made substantial contributions to the conception and design and acquisition and interpretation of data, took part in drafting the article and revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Ethical issues (including plagiarism, informed consent, misconduct, data fabrication and/or falsification, double publication and/or submission, and redundancy) have been completely observed by the authors.
Zheng J. SARS-CoV-2: an emerging coronavirus that causes a global threat. Int J Biol. 2020;16(10):1678.
WHO. WHO Coronavirus disease (COVID-19) dashboard [Internet]. 2021 [cited 2021 Jan 30]. Available from: https://covid19.who.int/table.
Zaim S, Chong JH, Sankarnarayanan V, et al. COVID-19 and multiorgan response. Curr Probl Cardiol. 2020;45(8):100618.
Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239-42.
Jayaweera M, Perera H, Gunawardana B, et al. Transmission of COVID-19 virus by droplets and aerosols: a critical review on the unresolved dichotomy. Enviro Res. 2020;188:109819.
Lu CW, Liu XF, Jia ZF. 2019-nCoV transmission through the ocular surface must not be ignored. Lancet. 2020;395(10224):e39.
Klompas M, Baker MA, Rhee C. Airborne transmission of SARS-CoV-2: theoretical considerations and available evidence. JAMA. 2020;324(5):441-2.
WHO. Rational use of personal protective equipment for coronavirus disease 2019 (COVID-19) [Internet]. 2020 [cited 2020 Oct 17]. Available from: https://apps.who.int/iris/bitstream/handle/10665/331215/WHO-2019-nCov-IPCPPE_use-2020.1-eng.pdf.
CDC. Interim infection prevention and control recommendations for healthcare personnel during the coronavirus disease 2019 (COVID-19) pandemic [Internet]. 2020 [cited 2020 Oct 16]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html.
ECDC. ECDC TECHNICAL REPORT. Infection prevention and control for COVID-19 in healthcare settings-first update [Internet]. 2020 [cited 2020 Oct 16]. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-infection-prevention-and-control-healthcare-settings-march-2020.pdf.
Muñoz-Leyva F, Niazi AU. Common breaches in biosafety during donning and doffing of protective personal equipment used in the care of COVID-19 patients. Can J Anesth. 2020;67(7):900-1.
WHO. Water, sanitation, hygiene, and waste management for SARS-CoV-2, the virus that causes COVID-19 [Internet]. 2020 [cited 2020 Oct 16]. Available from: https://www.who.int/publications/i/item/water-sanitation-hygiene-and-waste-management-for-the-covid-19-virus-interim-guidance.
Nakarmi M. Safe health care waste management practices in Nepal: lessons learned and challenges in the context of the COVID-19 Pandemic [Internet]. 2020 [cited 2020 Oct 16]. Available from: https://www.who.int/docs/default-source/searo/wsh-och-searo/mahesh-nakarmi-hecaf360-who-searo-june-25-2020-mahesh-nepal.pdf?sfvrsn=725ac527_4.
Government of Nepal Ministry of Health and Population. Health care waste management in the context of COVID-19 emergency (Interim Guidance) [Internet]. 2020 [cited 2020 Oct 16]. Available from: https://dwssm.gov.np/wp-content/uploads/2020/07/HCWM_COVID-19-Guidelines_En.pdf.
Singh N, Tang Y, Zhang Z, et al. COVID-19 waste management: effective and successful measures in Wuhan, China. Resour Conserv Recycl. 2020;163:105071.
Nzediegwu C, Chang SX. Improper solid waste management increases potential for COVID-19 spread in developing countries. Resour Conserv Recycl. 2020;161:104947.
Nguyen LH, Drew DA, Graham MS, et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. 2020;5(9):e475-83.
Singh N, Tang Y, Ogunseitan OA. Environmentally sustainable management of used personal protective equipment. Environ Sci Technol. 2020;54(14):8500-2.
Kumar J, Katto MS, Siddiqui AA, et al. Knowledge, attitude, and practices of healthcare workers regarding the use of face mask to limit the spread of the new coronavirus disease (COVID-19). Cureus. 2020;12(4):e7737.
Lyu W, Wehby GL. Community use of face masks and COVID-19: evidence from a natural experiment of State mandates in the US: study examines impact on COVID-19 growth rates associated with state government mandates requiring face mask use in public. Health Aff. 2020;39(8):1419-25.
Liu M, Cheng SZ, Xu KW, et al. Use of personal protective equipment against coronavirus disease 2019 by healthcare professionals in Wuhan, China: cross sectional study. BMJ. 2020;369:m2195.
Piché-Renaud PP, Groves HE, Kitano T, et al. Healthcare worker perception of a global outbreak of novel coronavirus (COVID-19) and personal protective equipment: survey of a pediatric tertiary-care hospital. Infect Control Hosp Epidemiol. 2020;1-7.
Ong JJY, Bharatendu C, Goh Y, et al. Headaches associated with personal protective equipment-a cross-sectional study among frontline healthcare workers during COVID-19. Headache. 2020;60(5):864-77.