Corresponding author: Naoyuki Sato, nsato@ncgg.go.jp
DOI: 10.31662/jmaj.2024-0153
Received: July 8, 2024
Accepted: December 17, 2024
Advance Publication: March 7, 2025
Published: April 28, 2025
Cite this article as:
Matsumoto S, Satoh T, Shinohara M, Kawano R, Suzuki K, Krell-Roesch J, Ide M, Watada H, Akishita M, Arai H, Kondo I, Geda YE, Sato N. Development of Modified Japanese Versions of Questionnaires to Assess Physical and Cognitively Stimulating Activities. JMA J. 2025;8(2):498-505.
Introduction: Lifestyle factors such as physical and cognitively stimulating activities may protect against various diseases. However, only a few simple and validated questionnaires assess the lifestyle factors in Japan. Thus, we aimed to create Japanese versions of such questionnaires for assessing physical and cognitively stimulating activities. This study examined their inter-rater reliability and test-retest reproducibility.
Methods: We developed a Japanese version of questionnaires by translating the English questionnaire that assesses the frequency of several physical and cognitively stimulating activities. Additionally, the Japanese version assesses the duration of engagement in physical activities, and we have added mental activities such as meditation and Zen practice. The inter-rater reliability and test-retest reproducibility of evaluating the frequency, duration, frequency × duration of each physical activity, and frequency of each cognitively stimulating activity were tested in healthy volunteers.
Results: The study included 48 participants aged 25-67 years. We observed good inter-rater reliability and test-retest reproducibility for the physical and cognitively stimulating activity questionnaires. As a pilot approach, we calculated the Total Physical Activity Score (metabolic equivalents·min/week) with an intraclass correlation coefficient (ICC) (2,1) of 0.818 (95% confidence interval, 0.698-0.894), indicating good test-retest reproducibility.
Conclusions: The Japanese versions of questionnaires used to assess the frequency and duration of physical and cognitively stimulating activities generally have good inter-rater reliability and test-retest reproducibility. While introducing the duration of engagement might enable the estimation of the Total Physical Activity Score, further validation using objective measures of activities and other self-reported physical activity questionnaires is necessary, which is a limitation of this study.
Key words: questionnaire, physical activities, cognitively stimulating activities, lifestyle, reliability
Lifestyle factors, such as physical and cognitively stimulating activities may impact various diseases, including geriatric diseases such as dementia, frailty, and vascular diseases (1), (2), (3), (4), (5), (6). Thus, surveys with validated questionnaires that measure lifestyle factors are critical proximal steps to potentially prevent diseases and promote health. However, only a few simple and validated questionnaires assess lifestyle factors in Japan(7), (8), (9), (10). Several questionnaires assessing the frequency of physical and cognitively stimulating activities were developed in English (11), (12) and have been used in research for examining the associations between lifestyle factors and the risk of mild cognitive impairment or dementia (13), (14), (15), (16), (17), (18), (19). Creating a Japanese version of the English questionnaires would enable future comparisons among studies conducted in different countries. The International Physical Activity Questionnaire (IPAQ) and the Global Physical Activity Questionnaire, GPAQ are available in Japanese and are used in research (20), (21); these questionnaires assess only the physical activities lasting for >10 min (9), (10). Although the Japan Arteriosclerosis Longitudinal Study Physical Activity Questionnaire was initially developed and well-validated in Japan, assessing physical activities lasting <10 min (22), its use in international collaborative studies may be challenging because there is no English version. The Japan Public Health Center-based Prospective Study Questionnaire compactly assesses the physical activities but not time (23).
Lifestyle factors substantially vary among different countries and cultures. Thus, creating culturally congruent questionnaires that match a country’s or cultural area’s lifestyle habits is necessary. Therefore, this study aimed to create Japanese versions of questionnaires used in the US to assess the frequency of engagement in physical and cognitively stimulating activities effectively and evaluate the Japanese version of the physical and cognitively stimulating activities questionnaires by examining the inter-rater reliability and test-retest reproducibility.
We translated two validated questionnaires used in the Mayo Clinic Study of Aging (MCSA) in Olmsted County, Minnesota, USA, for assessing the frequency of physical and cognitively stimulating activities in Japanese. The questionnaires were derived from two validated instruments, the 1985 National Health Interview Survey and the Minnesota Heart Survey intensity codes (24), (25). Three levels of physical activity and exercise intensity are distinguished by providing examples for each level: light physical activity (e.g., laundry, vacuuming, making beds, or dusting), moderate physical activity (e.g., scrubbing floors, washing windows, gardening, or raking leaves), heavy physical activity (e.g., carrying heavy objects, heavy digging, pushing a mower, or hard manual labor), light physical exercise (e.g., leisurely walking or slow dancing), moderate physical exercise (e.g., hiking or swimming), and vigorous physical exercise (e.g., jogging or playing singles tennis). In addition, participants were asked to indicate the frequency at which they performed these activities: ≤1 times per month, 2-3 times per month, 1-2 times per week, 3-4 times per week, 5-6 times per week, and daily. In the MCSA, the questionnaires are used to assess the physical activities performed by the participants during two time periods, i.e., in the last 12 months and when the participants were 50-65 years old. Reportedly, the physical activity questionnaire has moderate to good internal consistency, and the test-retest correlation coefficients was 0.33 for vigorous intensity activity and 0.50 for moderate intensity activity (11). Similar to the physical activity questionnaire, the questionnaire assessing cognitively stimulating activities inquired engaging in reading books, craft activities (e.g., knitting, quilting), computer use, playing games (e.g., puzzles, crosswords), and social activities (e.g., going out to movies and theaters) and assessed the frequency of engagement using the same categories as in the physical activities questionnaire (i.e., ≤1 times per month, 2-3 times per month, 1-2 times per week, 3-4 times per week, 5-6 times per week, and daily) (18). Several papers have been published based on both questionnaires(11), (12), (16), (18).
Because the lifestyle is different in Japan and the US, simply translating the English questionnaire into Japanese would hinder its widespread use. Therefore, we have made modifications to accommodate the differences in lifestyles between Japan and the US. The US version does not include items on the duration of engagement in physical and cognitively stimulating activities, making it difficult to quantitatively evaluate physical activity and exercise, e.g., by calculating energy expenditure using metabolic equivalents (METs). Therefore, we added an item to estimate the duration of physical activities. Furthermore, the frequencies of performing physical and cognitively stimulating activities in the US questionnaire were assessed through six categories, i.e., ≤1 times per month, 2-3 times per month, 1-2 times per week, 3-4 times per week, 5-6 times per week, and every day (11). As the Japanese way of thinking does not include “zero or none,” we created two separate categories of “none” and “≤1 per month” in the Japanese version. Finally, a new item on mental activities, such as meditation and Zen practice, was introduced in the questionnaire to assess the frequency of cognitively stimulating activities.
Two geriatricians translated the English questionnaires into Japanese, and two additional senior geriatricians reviewed the Japanese version. Next, the Japanese version was modified as described above. The back translation was performed by a Japanese translator―who graduated from a top-ranked University with >10 years of experience and EIKEN 1st grade (highest), which is Japan’s most widely recognized English language assessment―and double-checked by a native speaker who lived in North America. The back translation of examples of physical and cognitively stimulating activities is described in the Supplementary Methods and shown in Supplementary Figure 1 and 2 respectively.
The Clinical Research Ethics Committee of the National Center for Geriatrics and Gerontology approved this study (No. 1590-4). This study conforms to the provisions of the Declaration of Helsinki (revised in Tokyo in 2004). We examined the inter-rater reliability and test-retest reproducibility of the Japanese versions of the physical and cognitively stimulating activity questionnaires. A total of 30 Obu City employees, 10 Nishiki Memorial Hospital workers, and 8 Nakano Gastrointestinal Hospital workers provided written informed consent and participated in this study. The anonymity of the participants was also preserved. The participants were healthy volunteers. First, under the guidance of examiner A, the participants completed two questionnaires to assess physical and cognitively stimulating activities (Supplementary Figure 3 and 4). The examiner explained the general contents of the questionnaires to the participants and, while resolving doubts, if any, asked them to fill the questionnaires. The participants completed the same questionnaires on the same day under the guidance of examiner B. After 2 weeks, the participants completed the questionnaires under the guidance of examiner A. The inter-rater reliability was assessed by comparing the answers provided under examiner A’s and B’s guidance on day 1. The test-retest reproducibility was assessed by comparing the answers on day 1 and 2 weeks later, under the guidance of examiner A.
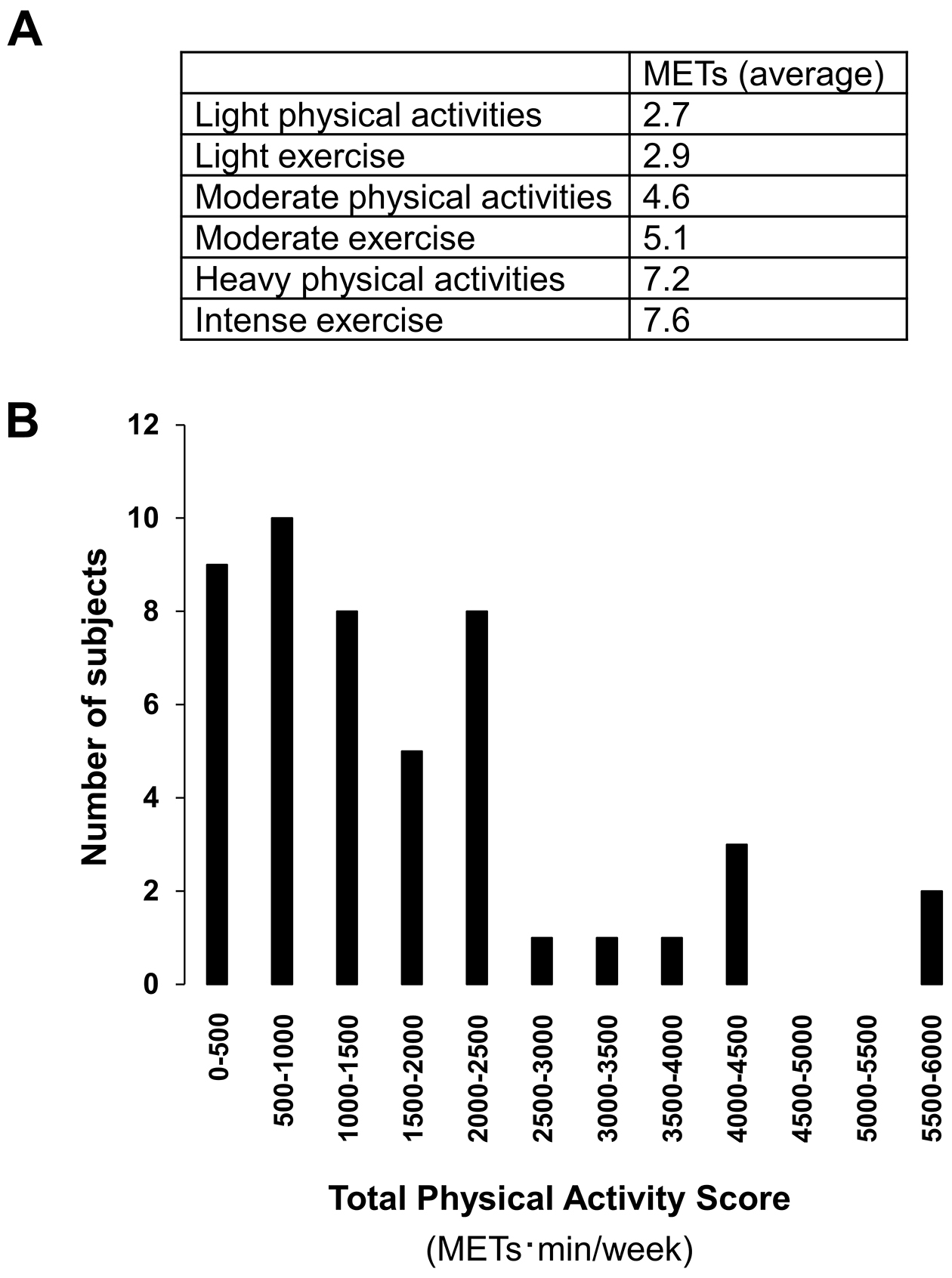
We calculated a Total Physical Activity Score (METs·min/week) using the physical activity questionnaire (Figure 1A). The Total Physical Activity Score reflects the sum of the METs for each self-reported physical activity or exercise multiplied by frequency per week (i.e., 0, ≤1 times per month, 2-3 times per month, 1-2 times per week, 3-4 times per week, 5-6 times per week, and every day) and duration per day when physical activity or exercise was performed (min). METs indicate physical activity intensity by estimating how much energy is consumed compared with resting (which is set at 1 MET) (26). MET values for each activity in the physical activity questionnaire are shown in Supplementary Table 1. Reportedly (11), the scores to indicate the frequency of engaging derived from the six response categories are 0 for none, 0.1 for ≤1 times per month, 0.5 for 2-3 times per month, 1.5 for 1-2 times per week, 3.5 for 3-4 times per week, 5.5 for 5-6 times per week, and 7 for daily. Thus, the formula for the Total Physical Activity Score (METs·min/week) was 2.7 (METs) × frequency of light physical activities (/week) × duration (min) + 2.9 (METs) × frequency of light exercise (/week) × duration (min) + 4.6 (METs) × frequency of moderate physical activities (/week) × duration (min) + 5.1 (METs) × frequency of moderate exercise (/week) × duration (min) + 7.2 (METs) × frequency of heavy physical activities (/week) × duration (min) + 7.6 (METs) × frequency of intense exercise (/week) × duration (min). Next, we examined the inter-rater reliability and test-retest reproducibility of the Total Physical Activity Score of each participant.
We performed statistical analyses using JMP Pro software (version 13, SAS Institute Inc.) or Excel 2021 (Microsoft Corp.). We calculated Cronbach’s alpha and Spearman’s rank correlation coefficients to examine the inter-rater consistency between two examiners, and intraclass correlation and Spearman’s rank correlation coefficients to examine the reproducibility of test-retest between the two testing sessions (in an interval of 2 weeks) (27). Intraclass correlation coefficient (ICC) estimates and their 95% confidence intervals (CIs) were calculated based on a two-way random-effects model, single measurement, and absolute agreement (ICC(2.1)).
Based on the 95% CI of the ICC estimate, values <0.5, 0.5-0.75, 0.75-0.9, and >0.9 indicate poor, moderate, good, and excellent reliability, respectively (27). We considered p < 0.05 as statistically significant.
The study included 48 participants aged 25-67 years (mean ± SD age, 49.8 ± 11.7 years; 28 men and 20 women). The results of the inter-rater reliability of the physical activity questionnaire are summarized in Table 1 (left side). The Cronbach’s alpha coefficients for the frequencies/durations/and frequency × duration were as follows: light physical activity (0.971/0.955/0.951), light exercise (0.977/0.982/0.982), moderate physical activities (0.969/0.963/0.996), moderate exercise (0.972/0.914/0.985), heavy physical activity (0.838/0.948/0.997), and intense exercise (0.979/0.975/0.995). The Spearman’s rank correlations also agreed with the results of the Cronbach’s alpha coefficient analyses. Overall, these results showed good inter-rater reliability concerning frequency, duration, and frequency × duration of the physical activity questionnaire.
Table 1. Inter-Rater Reliability and Test-Retest Reproducibility of the Physical Activity Questionnaire.
| Inter-rater reliability | Test-retest reproducibility | ||||||
|---|---|---|---|---|---|---|---|
| Cronbach’s alpha coefficient | Spearman’s rank correlation | ICC (2,1) | Spearman’s rank correlation | ||||
| rho | p-value | rho | p-value | ||||
| Frequency | Light physical activity | 0.971 | 0.944 | <0.0001 | 0.847 (0.743, 0.912) | 0.825 | <0.0001 |
| Light exercise | 0.977 | 0.972 | <0.0001 | 0.854 (0.753, 0.916) | 0.853 | <0.0001 | |
| Moderate physical activity | 0.969 | 0.744 | <0.0001 | 0.933 (0.883, 0.962) | 0.704 | <0.0001 | |
| Moderate exercise | 0.972 | 0.964 | <0.0001 | 0.684 (0.498, 0.810) | 0.819 | <0.0001 | |
| Heavy physical activity | 0.838 | 0.953 | <0.0001 | 0.792 (0.656, 0.878) | 0.822 | <0.0001 | |
| Intense exercise | 0.979 | 0.905 | <0.0001 | 0.379 (0.113, 0.595) | 0.576 | <0.0001 | |
| Average duration per day (min) | Light physical activities | 0.955 | 0.904 | <0.0001 | 0.874 (0.786, 0.928) | 0.827 | <0.0001 |
| Light exercise | 0.982 | 0.906 | <0.0001 | 0.930 (0.879, 0.960) | 0.823 | <0.0001 | |
| Moderate physical activity | 0.963 | 0.836 | <0.0001 | 0.850 (0.747, 0.913) | 0.600 | <0.0001 | |
| Moderate exercise | 0.914 | 0.896 | <0.0001 | 0.762 (0.611, 0.859) | 0.774 | <0.0001 | |
| Heavy physical activity | 0.948 | 0.951 | <0.0001 | 0.205 (−0.084, 0.462) | 0.786 | <0.0001 | |
| Intense exercise | 0.975 | 0.889 | <0.0001 | 0.768 (0.623, 0.863) | 0.596 | <0.0001 | |
| Frequency × Duration | Light physical activity | 0.951 | 0.894 | <0.0001 | 0.861 (0.765, 0.920) | 0.818 | <0.0001 |
| Light exercise | 0.982 | 0.955 | <0.0001 | 0.576 (0.348, 0.739) | 0.824 | <0.0001 | |
| Moderate physical activity | 0.996 | 0.793 | <0.0001 | 0.990 (0.983, 0.995) | 0.749 | <0.0001 | |
| Moderate exercise | 0.985 | 0.968 | <0.0001 | 0.965 (0.938, 0.980) | 0.824 | <0.0001 | |
| Heavy physical activity | 0.997 | 0.953 | <0.0001 | 0.385 (0.112, 0.602) | 0.802 | <0.0001 | |
| Intense exercise | 0.995 | 0.913 | <0.0001 | 0.576 (0.353, 0.737) | 0.583 | <0.0001 | |
| Regular programs | 1 | 1 | 1 | <0.0001 | 1 (1, 1) | 1 | |
| ICC (2, 1) is presented as the coefficient with a 95% confidence interval. ICC, intraclass correlation coefficient |
|||||||
The results of the test-retest reproducibility of the physical activity questionnaire are summarized in Table 1 (right side). The ICC (2,1) values for the frequencies/durations/and frequency × duration were as follows: light physical activity (0.847/0.874/0.861), light exercise (0.854/0.930/0.576), moderate physical activities (0.933/0.850/0.990), moderate exercise (0.684/0.762/0.965), heavy physical activity (0.792/0.205/0.385), and intense exercise (0.379/0.768/0.576). Moreover, all items were statistically significant in the Spearman’s rank correlation analyses. Overall, the test-retest reproducibility for the frequency, duration, and frequency × duration of the physical activity questionnaire had moderate to excellent reliabilities, except for duration and frequency × duration of heavy physical activities and the frequency of intense exercise, although the Spearman’s rank correlations were statistically significant.
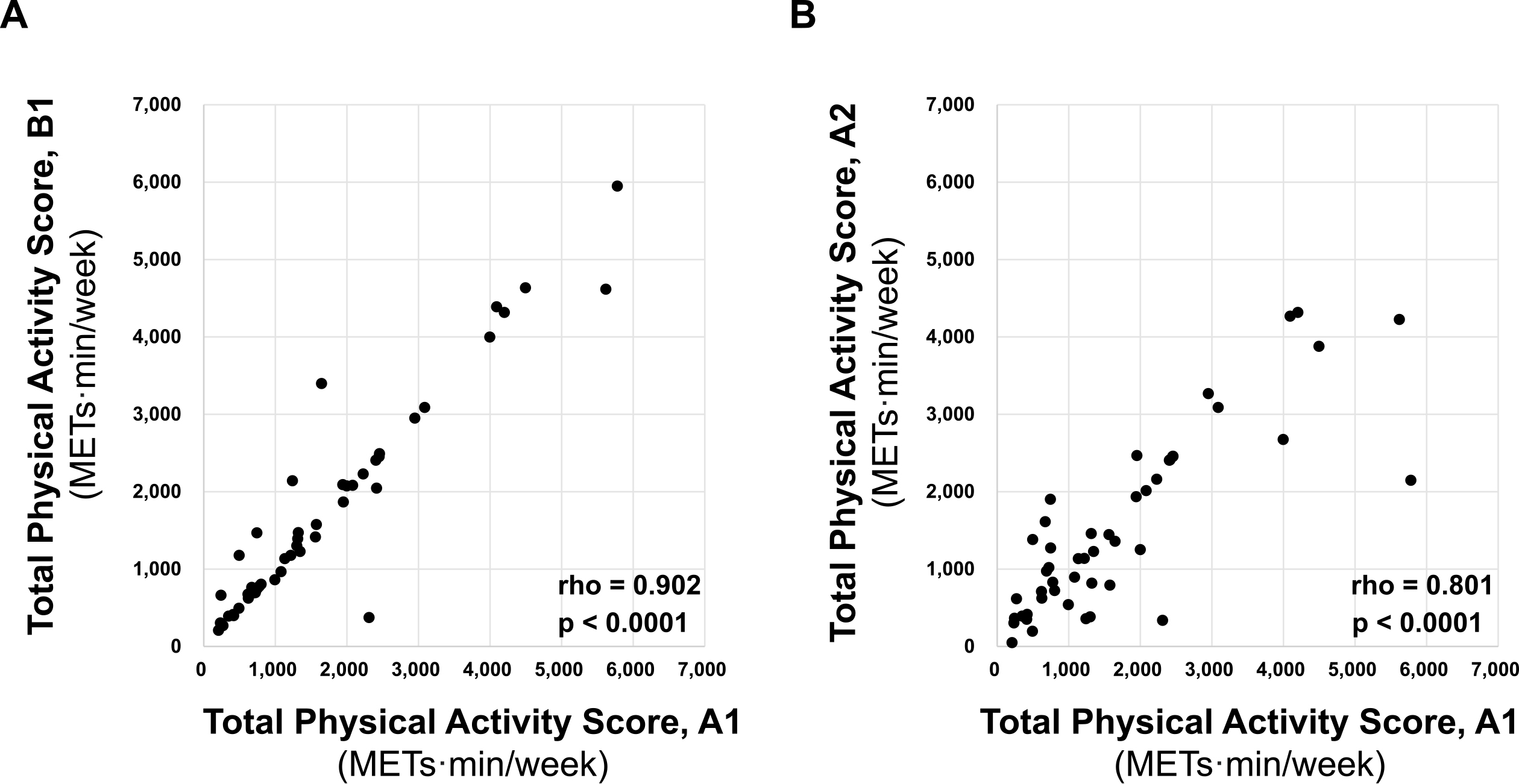
Figure 1B displays the distribution of Total Physical Activity Score (METs·min/week) using the physical activity questionnaire. The Cronbach’s alpha coefficient for the inter-rater reliability of the Total Physical Activity Score was 0.971; the ICC (2,1) value to indicate test-retest reproducibility was 0.818 (95% CI, 0.698-0.894). Moreover, the Spearman’s rank correlation showed that the inter-rater reliability and test-retest reproducibility of the score were well retained (r = 0.902, p < 0.0001, and r = 0.801, p < 0.0001, respectively) (Figure 2A and B). While analyzing >55 years old participants (n = 18), we observed good inter-rater reliability and test-retest reproducibility (Supplementary Figure 6). Additionally, when separated by sex, there were still good inter-rater reliability and test-retest reproducibility (Supplementary Figure 7). Overall, these results indicate good inter-rater reliability and test-retest reproducibility for the Total Physical Activity Score.
Finally, the Cronbach’s alpha coefficients to indicate the inter-rater reliability for the frequencies of reading newspapers, reading magazines, reading books, playing games, playing music by yourself, artistic activity, mental activity, handicraft, group activity, social activity, using a computer (including smartphone), and television were 0.990, 0.929, 0.928, 0.930, 0.926, 0.999, 1.000, 0.929, 0.884, 0.873, 0.898, and 0.986, respectively (Table 2). The Spearman’s rank correlation coefficients indicating the inter-rater reliability of the cognitively stimulating activity questionnaire were good. The ICC (2,1) to indicate test-retest reproducibility for the frequencies of reading newspapers, reading magazines, reading books, playing games, playing music by yourself, artistic activity, mental activity, handicraft, group activity, social activity, using a computer (including smartphone), and television were 0.974, 0.904, 0.857, 0.823, 0.947, 1, 0.994, 0.994, 0.737, 0.668, 0.667, and 0.862, respectively (Table 2). These results indicate that the test-retest reproducibility for the cognitively stimulating activities was moderate to excellent. Overall, these data suggest that the questionnaire used to assess cognitively stimulating activities had good inter-rater reliability and test-retest reproducibility.
Table 2. Inter-Rater reliability and Test-Retest Reproducibility of the Cognitively Stimulating Activity Questionnaire.
| Inter-rater reliability | Test-retest reproducibility | |||||
|---|---|---|---|---|---|---|
| Cronbach's alpha coefficient | Spearman's rank correlation | ICC (2,1) | Spearman's rank correlation | |||
| rho | p-value | rho | p-value | |||
| Reading newspapers | 0.990 | 0.978 | <0.0001 | 0.974 (0.954, 0.985) | 0.979 | <0.0001 |
| Reading magazines | 0.929 | 0.844 | <0.0001 | 0.904 (0.835, 0.945) | 0.816 | <0.0001 |
| Reading books | 0.928 | 0.922 | <0.0001 | 0.857 (0.759, 0.917) | 0.857 | <0.0001 |
| Playing games | 0.930 | 0.985 | <0.0001 | 0.823 (0.706, 0.897) | 0.871 | <0.0001 |
| Playing music by yourself | 0.926 | 0.846 | <0.0001 | 0.947 (0.907, 0.970) | 0.846 | <0.0001 |
| Artistic activities | 0.999 | 1.000 | <0.0001 | 1 (1, 1) | 1.000 | <0.0001 |
| Mental activities | 1.000 | 0.937 | <0.0001 | 0.994 (0.989, 0.996) | 1.000 | <0.0001 |
| Handicraft | 0.929 | 0.877 | <0.0001 | 0.994 (0.990, 0.997) | 0.899 | <0.0001 |
| Group activities | 0.884 | 0.937 | <0.0001 | 0.737 (0.577, 0.843) | 0.691 | <0.0001 |
| Social activities | 0.873 | 0.723 | <0.0001 | 0.668 (0.475, 0.800) | 0.743 | <0.0001 |
| Using a computer (including smartphone) | 0.898 | 0.939 | <0.0001 | 0.667 (0.478, 0.798) | 0.773 | <0.0001 |
| Television | 0.986 | 0.927 | <0.0001 | 0.862 (0.767, 0.920) | 0.889 | <0.0001 |
| ICC (2, 1) is presented as the coefficient with a 95% confidence interval. ICC, intraclass correlation coefficient |
||||||
We obtained good inter-rater reliability and test-retest reproducibility for the physical and cognitively stimulating activity questionnaires. Furthermore, as adding the duration of each session to the physical activity questionnaire helped estimate the total amount of physical activity, we calculated a Total Physical Activity Score using METs and observed its good inter-rater reliability and test-retest reproducibility.
Possible uses of these questionnaires include research (e.g., epidemiological, observational, intervention, and clinical studies), general practice, health checkups, individual use, and national and local government use, while these questionnaires still need some validation in Japanese. The questionnaires can be retrieved from the corresponding author upon request. The Japanese versions are also provided as supplemental materials. The questionnaires can also be used in general hospitals for everyday medical care and serve as a basis for communication between patients and clinicians. Obtaining information on patients’ engagement in physical and cognitively stimulating activities using these questionnaires can help clinicians provide feedback to the patients (e.g., on healthy lifestyle choices). The questionnaires can also be used for health checkups, for example, in middle-aged individuals, and for repeated measurements to track changes in patients’ engagement in physical and cognitively stimulating activities over time. Individual use may facilitate self-evaluation and reflection. Moreover, the questionnaires may be useful for citizen surveys by national and local governments or other stakeholders to inform policies or guidelines. Finally, investigating lifestyle factors over the course of a lifetime may prevent and treat various diseases (28), (29), (30), (31), (32), (33).
The limitations of this study are the small sample size and the convenience sample of healthy volunteer participants, in addition to the study population being biased. The participants’ ages were 25-67 years. Their occupational backgrounds were also skewed, with a high proportion of healthcare workers. Furthermore, the validity of the Total Physical Activity Score was not assessed. Future research is critically needed to examine the correlation between the Total Physical Activity Score obtained using this questionnaire and objective measures of physical activities, such as doubly labeled water (8) or accelerometry, to further validate the physical activity questionnaire.
A standard protocol for calculating total energy expenditure using several physical activity questionnaires used in Japanese cohort studies is also under consideration (34). GPAQ and IPAQ measure physical activities and exercises only when performed for >10 min (9), (10). The physical activity questionnaire provided herein inquires any physical activity and exercise, including those performed for <10 min, and thus might contribute to establishing this standard protocol. Another strength of this study is that we added “mental activities” such as “meditation,” “Zen―a Japanese form of Buddhism,” “prayer,” and “sutra chanting,” to the Japanese version of the questionnaire on the frequency of cognitively stimulating activities, even though these items were not included in the US questionnaire. Therefore, the Japanese version of the questionnaire is suitable to the Japanese culture, potentially contributing to the widespread use of this questionnaire in Japan.
In conclusion, the Japanese questionnaires used to assess physical and cognitively stimulating activities have good inter-rater reliability and test-retest reproducibility. The physical activity questionnaire requires further validation using objective measures of activities and other self-reported physical activity questionnaires. Because we have made culturally congruent modifications, such as adding mental activities including meditation and Zen practice, it will be helpful for Asians and other countries to create their national language versions based on this Japanese version.
None
This work was supported in part by the Research Funding for Longevity Sciences from NCGG (19-3 & 21-12 to NS).
We thank Ms. Mika Kitagawa, Mr. Hiroshi Nakamura, and the study participants at the Obu City Municipal Office, Nishiki Memorial Hospital, and Nakano Gastrointestinal Hospital for their contribution. We express our gratitude to the members of the Department of Aging Neurobiology, the Innovation Center for Translational Research in the National Center for Geriatrics and Gerontology, the staff of Nishiki Memorial Hospital and Nakano Gastrointestinal Hospital for their help, and Dr. Yoshihiko Naito of Mukogawa Women’s University for the helpful discussions.
Conceptualization: NS and YEG; Data curation: NS, SM, TS, and MS; Formal analysis: NS, TS, MS, RK, and KS; Funding acquisition: NS; Investigation: NS, SM, TS, MS, and MI; Methodology: NS, SM, MS, JKR, HA, IK, and YEG; Supervision: HW, MA, HA, IK, and YEG; Writing: NS, SM, MS, JKR, and YEG. Shoya Matsumoto,Tomomi Satoh and Mitsuru Shinohara contributed equally to this work.
Masahiro Akishita is one of the Editors of JMA Journal and on the journal’s Editorial Staff. He was not involved in the editorial evaluation or decision to accept this article for publication at all.
Moller A, Mortensen OS, Reventlow S, et al. Lifetime occupational physical activity and musculoskeletal aging in middle-aged men and women in denmark: retrospective cohort study protocol and methods. JMIR Res Protoc. 2012;1(2):e7.
van de Laar RJ, Ferreira I, van Mechelen W, et al. Habitual physical activity and peripheral arterial compliance in young adults: the Amsterdam growth and health longitudinal study. Am J Hypertens. 2011;24(2):200-8.
Vemuri P, Lesnick TG, Przybelski SA, et al. Association of lifetime intellectual enrichment with cognitive decline in the older population. JAMA Neurol. 2014;71(8):1017-24.
Vemuri P, Lesnick TG, Przybelski SA, et al. Effect of intellectual enrichment on AD biomarker trajectories: longitudinal imaging study. Neurology. 2016;86(12):1128-35.
Verweij LM, van Schoor NM, Deeg DJ, et al. Physical activity and incident clinical knee osteoarthritis in older adults. Arthritis Rheum. 2009;61(2):152-7.
Gow AJ, Pattie A, Deary IJ. Lifecourse activity participation from early, mid, and later adulthood as determinants of cognitive aging: the Lothian birth cohort 1921. J Gerontol B Psychol Sci Soc Sci. 2017;72(1):25-37.
Tsugane S, Sawada N. The JPHC study: design and some findings on the typical Japanese diet. Jpn J Clin Oncol. 2014;44(9):777-82.
Ishikawa-Takata K, Naito Y, Tanaka S, et al. Use of doubly labeled water to validate a physical activity questionnaire developed for the Japanese population. J Epidemiol. 2011;21(2):114-21.
Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381-95.
World Health Organization [Internet]. GPAQ analysis guide. [cited 2024 Jun 27]. Available from: https://www.who.int/docs/default-source/ncds/ncd-surveillance/gpaq-analysis-guide.pdf.
Geda YE, Roberts RO, Knopman DS, et al. Physical exercise, aging, and mild cognitive impairment: a population-based study. Arch Neurol. 2010;67(1):80-6.
Geda YE, Topazian HM, Roberts LA, et al. Engaging in cognitive activities, aging, and mild cognitive impairment: a population-based study. J Neuropsychiatry Clin Neurosci. 2011;23(2):149-54.
Krell-Roesch J, Syrjanen JA, Vassilaki M, et al. Association of non-exercise physical activity in mid- and late-life with cognitive trajectories and the impact of APOE epsilon4 genotype status: the Mayo clinic study of aging. Eur J Ageing. 2019;16(4):491-502.
Krell-Roesch J, Pink A, Roberts RO, et al. Timing of physical activity, apolipoprotein E epsilon4 genotype, and risk of incident mild cognitive impairment. J Am Geriatr Soc. 2016;64(12):2479-86.
Krell-Roesch J, Feder NT, Roberts RO, et al. Leisure-time physical activity and the risk of incident dementia: the Mayo clinic study of aging. J Alzheimers Dis. 2018;63(1):149-55.
Krell-Roesch J, Syrjanen JA, Bezold J, et al. Physical activity and trajectory of cognitive change in older persons: Mayo clinic study of aging. J Alzheimers Dis. 2021;79(1):377-88.
Vassilaki M, Cha RH, Aakre JA, et al. Mortality in mild cognitive impairment varies by subtype, sex, and lifestyle factors: the Mayo clinic study of aging. J Alzheimers Dis. 2015;45(4):1237-45.
Krell-Roesch J, Vemuri P, Pink A, et al. Association between mentally stimulating activities in late life and the outcome of incident mild cognitive impairment, with an analysis of the APOE epsilon4 genotype. JAMA Neurol. 2017;74(3):332-8.
Vemuri P, Knopman DS, Lesnick TG, et al. Evaluation of amyloid protective factors and Alzheimer disease neurodegeneration protective factors in elderly individuals. JAMA Neurol. 2017;74(6):718-26.
Yamada K, Yamaguchi S, Sato K, et al. The COVID-19 outbreak limits physical activities and increases sedentary behavior: a possible secondary public health crisis for the elderly. J Orthop Sci. 2020;25(6):1093-4.
Shimizu Y, Tsuji K, Ochi E, et al. Study protocol for a nationwide questionnaire survey of physical activity among breast cancer survivors in Japan. BMJ Open. 2020;10(1):e032871.
Ishikawa-Takata K, Naito Y, Tanaka S, et al. Use of doubly labeled water to validate a physical activity questionnaire developed for the Japanese population. J Epidemiol. 2011;21(2):114-21.
Inoue M, Iso H, Yamamoto S, et al. Daily total physical activity level and premature death in men and women: results from a large-scale population-based cohort study in Japan (JPHC study). Ann Epidemiol. 2008;18(7):522-30.
Folsom AR, Caspersen CJ, Taylor HL, et al. Leisure time physical activity and its relationship to coronary risk factors in a population-based sample. The Minnesota heart survey. Am J Epidemiol. 1985;121(4):570-9.
Moss AJ, Parsons VL. Current estimates from the National Health Interview Survey. United States, 1985. Vital Health Stat 10. 1986;(160):i-iv, 1-182.
Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 Compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43(8):1575-81.
Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155-63.
van Sluijs EMF, Ekelund U, Crochemore-Silva I, et al. Physical activity behaviours in adolescence: current evidence and opportunities for intervention. Lancet. 2021;398(10298):429-42.
Middlekauff M, Lee W, Egger MJ, et al. Physical activity patterns in healthy middle-aged women. J Women Aging. 2016;28(6):469-76.
Turner MJ, Schmitt EE, Hubbard-Turner T. Weekly physical activity levels of older adults regularly using a fitness facility. J Aging Res. 2016;2016:5010285.
Reas ET, Laughlin GA, Bergstrom J, et al. Lifetime physical activity and late-life cognitive function: the Rancho Bernardo study. Age Ageing. 2019;48(2):241-6.
Boisvert-Vigneault K, Payette H, Audet M, et al. Relationships between physical activity across lifetime and health outcomes in older adults: results from the NuAge cohort. Prev Med. 2016;91:37-42.
Peels DA, Hoogenveen RR, Feenstra TL, et al. Long-term health outcomes and cost-effectiveness of a computer-tailored physical activity intervention among people aged over fifty: modelling the results of a randomized controlled trial. BMC Public Health. 2014;14:1099.
Nakata Y, Sasai H, Murakami H, et al. Scoring protocol for calculation of total energy expenditure by physical activity questionnaires used in Japanese cohort studies. Res Exerc Epidemiol. 2017;19(2):83-92. Japanese.
