Corresponding author: Tatsuya Maegawa, tmaegawa430@hotmail.com
DOI: 10.31662/jmaj.2024-0394
Received: December 3, 2024
Accepted: April 1, 2025
Advance Publication: May 30, 2025
Published: July 15, 2025
Cite this article as:
Maegawa T, Okumura E, Kohara K, Hashimoto R, Kubota M. Full-endoscopic Removal of a Lumbar Synovial Cyst after Laminectomy for Lumbar Spinal Canal Stenosis. JMA J. 2025;8(3):992-995.
Key words: full-endoscopic laminectomy, full-endoscopic spinal surgery, synovial cyst
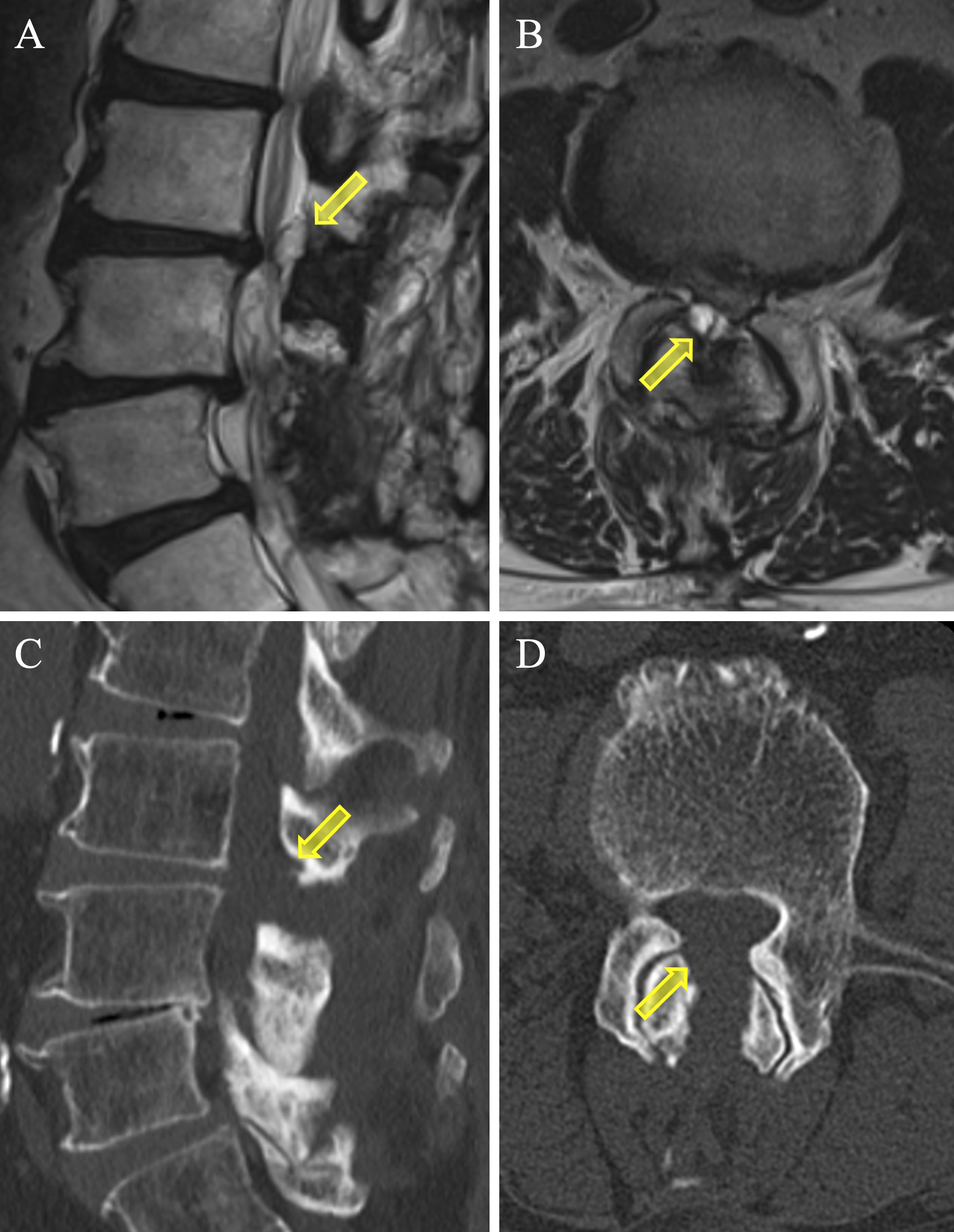
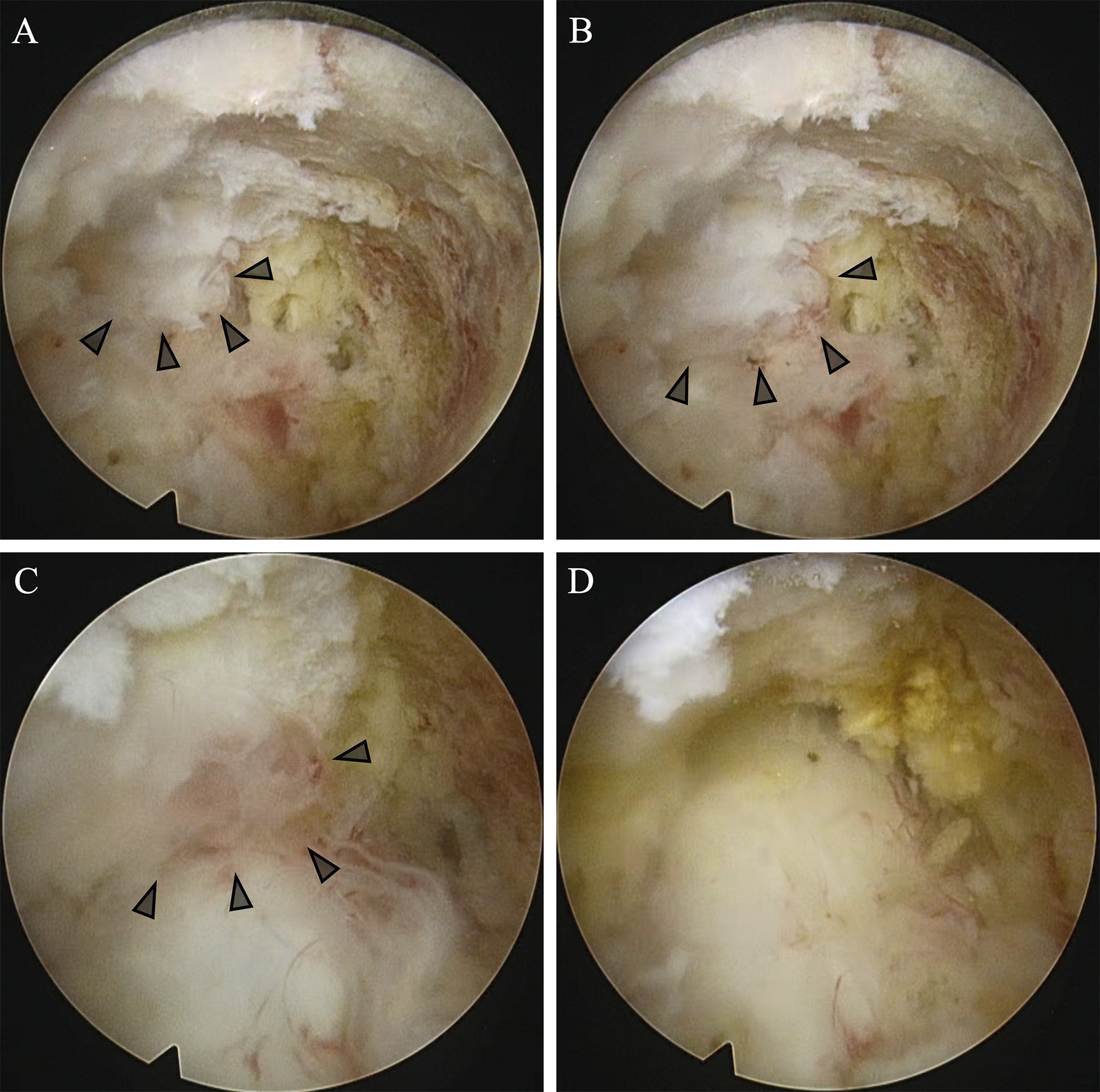
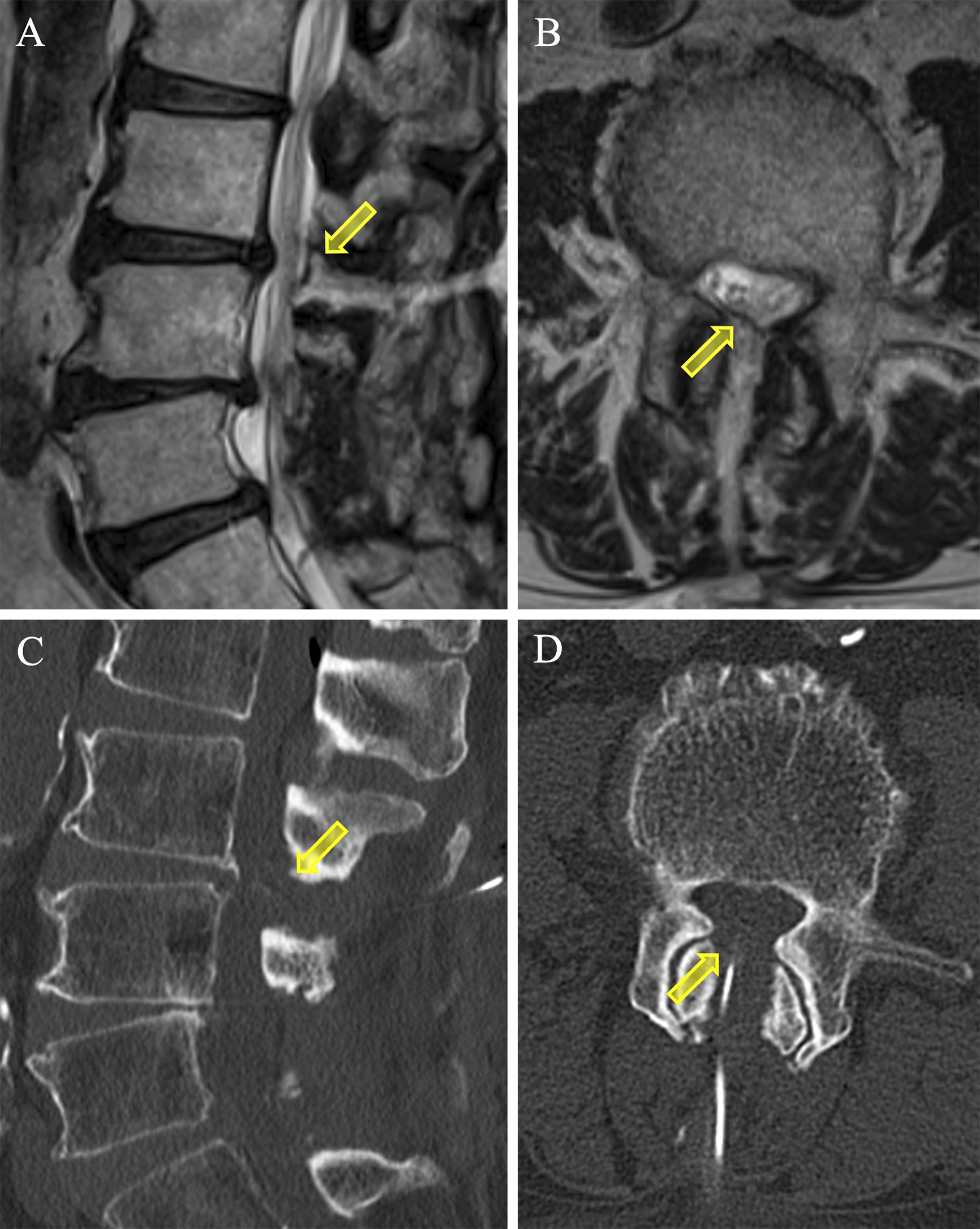
An 84-year-old man with a history of percutaneous coronary intervention, anticoagulation therapy for atrial fibrillation, and corticosteroid use for nephrotic syndrome presented with recurrent lumbar spinal stenosis. Two years earlier, he had undergone decompression surgery at L3/4/5/S1, followed by a repeat procedure one year later owing to recurrence. Despite initial relief, intermittent claudication returned. Magnetic resonance imaging (MRI) and computed tomography (CT) revealed re-stenosis at L3/4 caused by a synovial cyst (Figure 1). Considering his comorbidities, minimally invasive full-endoscopic spine surgery (FESS) was performed. Intraoperatively, the synovial cyst with respiratory pulsations was excised through additional fenestration (Figure 2). Postoperative MRI and CT confirmed adequate decompression, and the patient’s symptoms resolved, achieving an excellent outcome per MacNab criteria (Figure 3).
Synovial cysts, often associated with instability, degenerative spondylolisthesis, and facet joint arthritis, are rare, comprising 5% of cases (1), (2), (3). To the best of our knowledge, this is the first reported case of FESS for a postoperative synovial cyst, indicating its safety and potential for wider clinical application (3), (4), (5).
None
We thank Editage (www.editage.jp) for English language editing.
23-005-240411, institutional review board in Kameda Medical Center.
When reporting these cases, care was taken to protect the patient’s personal information and privacy, and consent was obtained from the patient for publication of the details contained herein.
Written informed consent was obtained from the patient to publish this case, including pictures.
Hellinger S, Lewandrowski KU. Clinical outcomes with endoscopic resection of lumbar extradural cysts. J Spine Surg. 2020;6(suppl 1):S133-44.
Giordan E, Gallinaro P, Stafa A, et al. A systematic review and meta-analysis of outcomes and adverse events for Juxtafacet cysts treatment. Int J Spine Surg. 2022;16(1):124-38.
Tacconi L, Spinelli R, Serra G, et al. Full-endoscopic removal of lumbar Juxtafacet cysts: a prospective multicentric study. World Neurosurg. 2020;141:e414-22.
Badra M, Najjar E, Wardani H, et al. Evaluation and treatment of lumbar spine extradural cysts: a narrative review. Cureus. 2024;16(5):e60604.
Leyendecker J, Sofoluke N, Hofstetter CP, et al. Full endoscopic resection of large bilateral synovial cysts in lumbar spine. Neurosurg Focus Video. 2024;10(2):V7.
