Corresponding author: Takashi Nawata, tnawata@yamaguchi-u.ac.jp
DOI: 10.31662/jmaj.2025-0019
Received: January 13, 2025
Accepted: February 17, 2025
Advance Publication: May 26, 2025
Published: July 15, 2025
Cite this article as:
Nawata T, Toyoshige M, Sano M. Diffuse Polyenthesitis after Intravesical Bacillus Calmette-Guerin Therapy. JMA J. 2025;8(3):984-985.
Key words: diffuse polyenthesitis, intravesical Bacillus Calmette-Guerin therapy, 18F-fluorodeoxyglucose positron emission tomography/computed tomography
A 72-year-old Japanese man experienced pain in the extremities and bilateral leg swelling. He had a history of bladder carcinoma and underwent intravesical Bacillus Calmette-Guerin (BCG) therapy. Two months after the last intravesical BCG therapy, the patient noticed the pain and presented at the outpatient clinic.
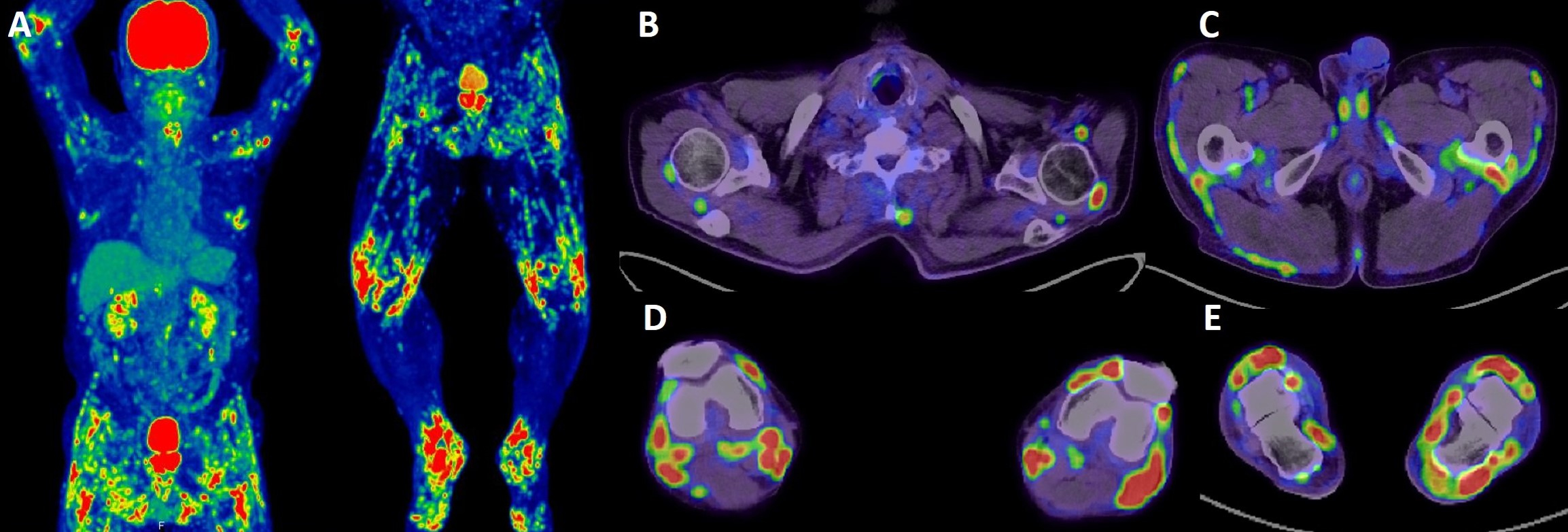
Laboratory examination showed elevated serum C-reactive protein levels (CRP: 1.48 mg/dL; normal range: below 0.14 mg/dL), normal serum matrix metalloproteinase-3 levels, and negative anti-citrullinated proteins antibodies and rheumatoid factor and antinuclear antibodies; 18F-fluorodeoxyglucose positron emission tomography/computed tomography showed fluorodeoxyglucose accumulation in a broad range of muscle-tendon attachment sites (Figure 1). The patient was diagnosed with diffuse polyenthesitis relevant to intravesical BCG therapy. However, 4 months after the last intravesical BCG therapy, his pain symptoms showed spontaneous remission, and serum levels of CRP decreased to 0.23 mg/dL.
Our case suggests the importance of recognizing that intravesical BCG therapy can be a cause of polyenthesitis (1).
None
Takashi Nawata was responsible for the conceptualization, methods, and writing―original draft. Michihiro Toyoshige and Motoaki Sano undertook the supervision and approved the final version to be submitted.
Our institution does not require ethical approval for reporting individual cases or case series. Written informed consent was obtained from the patient for publication of this report.
Bernini L, Manzini CU, Giuggioli D, et al. Reactive arthritis induced by intravesical BCG therapy for bladder cancer: our clinical experience and systematic review of the literature. Autoimmun Rev. 2013;12(12):1150-9.
