Corresponding author: Maiko Awashima, maiko.y.716@gmail.com
DOI: 10.31662/jmaj.2025-0093
Received: February 20, 2025
Accepted: March 11, 2025
Advance Publication: May 30, 2025
Published: July 15, 2025
Cite this article as:
Awashima M, Kichikawa Y, Suzuki K, Horikoshi H. Necrotizing Pneumonia Caused by Community-acquired Methicillin-resistant Staphylococcus aureus Following Influenza. JMA J. 2025;8(3):988-989.
Key words: community-acquired methicillin-resistant Staphylococcus aureus, CA-MRSA, CA-MRSA pneumonia, necrotizing pneumonia
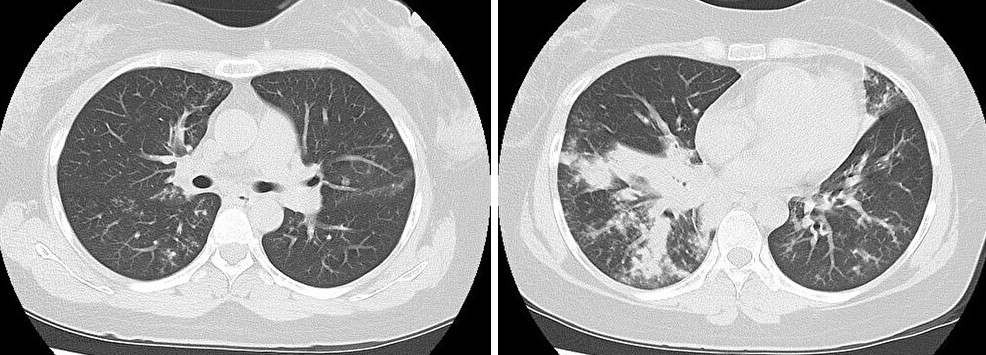
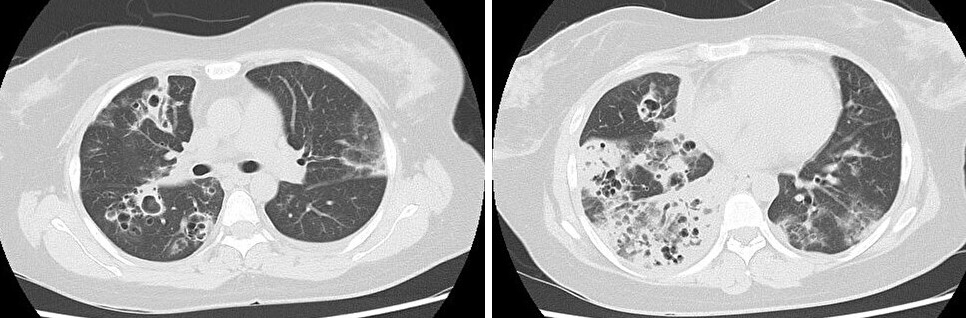
A 39-year-old female was presented to our hospital with fever, dyspnea, and chest pain. She had been diagnosed with influenza virus infection and had received antiviral drugs two days earlier. Despite this, she experienced difficulty maintaining adequate oxygenation on room air. She was administered oxygen using a reservoir mask at 15 L/min. Chest computed tomography (CT) revealed bilateral infiltrates (Figure 1), and methicillin-resistant Staphylococcus aureus (MRSA) was detected in her sputum. By the 10th day of hospitalization, chest CT showed multiple cavitary lesions (Figure 2). She was diagnosed with necrotizing pneumonia caused by community-acquired MRSA (CA-MRSA) (1). Following the administration of Linezolid, her clinical condition improved. In Japan, reports of CA-MRSA pneumonia are rare, but most of them involve severe pneumonia with the destruction of lung tissue. Unlike healthcare-associated MRSA pneumonia, CA-MRSA pneumonia has a tendency for cavitation within infiltrates (2). Therefore, it is necessary to include CA-MRSA pneumonia in the differential diagnosis when encountering pneumonia with multiple cavitary lesions.
None
Maiko Awashima wrote the manuscript, and the other authors revised it.
This study did not require IRB approval.
Consent was obtained from the patient.
Naimi TS, LeDell KH, Como-Sabetti K, et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA. 2003;290(22):2976-84.
Defres S, Marwick C, Nathwani D. MRSA as a cause of lung infection including airway infection, community acquired pneumonia and hospital-acquired pneumonia. Eur Respir J. 2009;34(6):1470-6.
