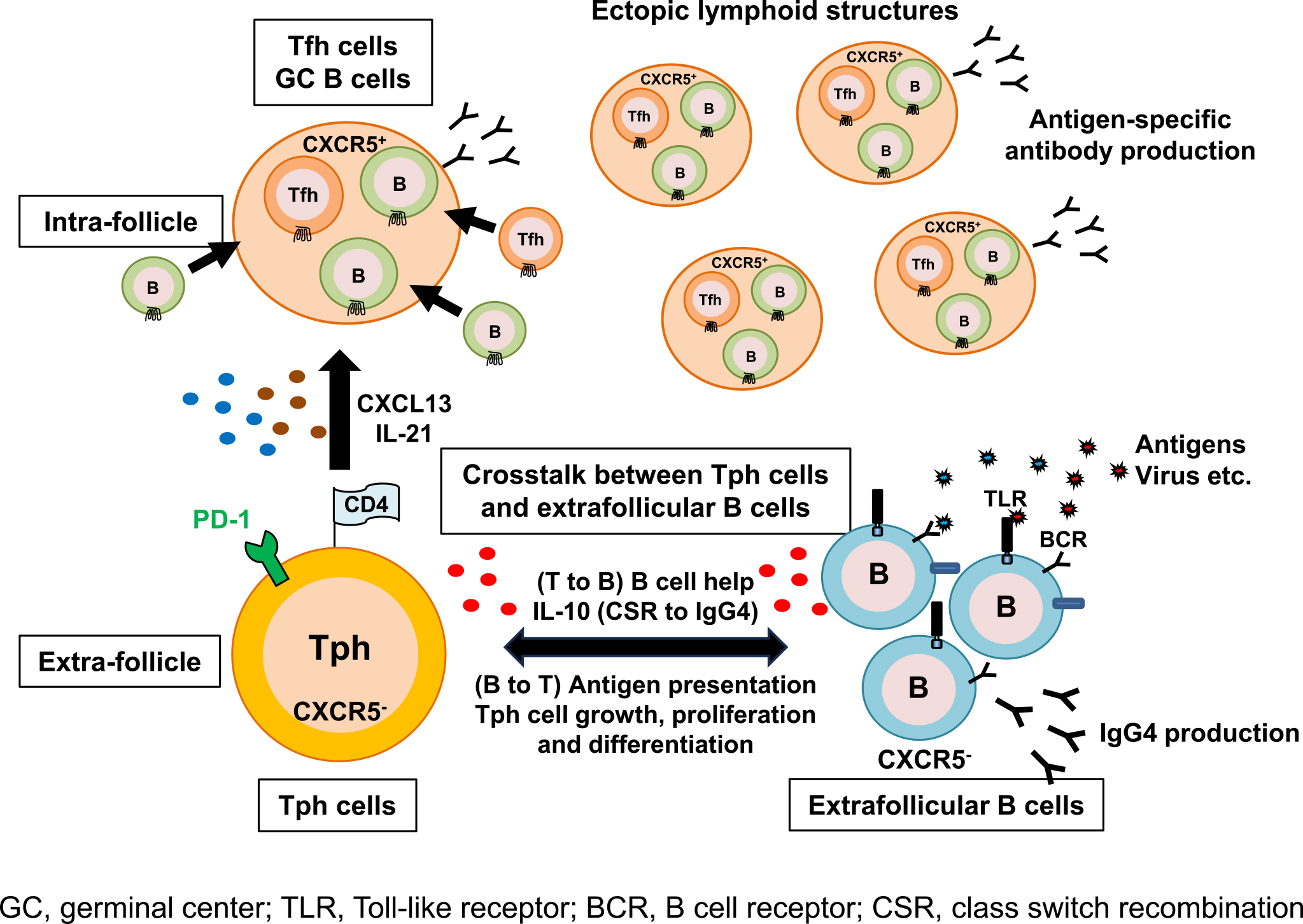
Figure 1. Histopathology of IgG4-related disease.
A: Formation of ectopic lymphoid structures (arrows) in a submandibular gland from a patient with IgG4-related dacryoadenitis and sialoadenitis. (b) High-magnification image of the dotted square area in (a). A section of the submandibular gland was stained via hematoxylin and eosin. Scale bars are 100 μm.
B: Immunohistochemistry staining for CD4 (brown). High-magnification images (b, intrafollicle; c, extrafollicle) of the dotted square areas in low-magnification image (a). Hematoxylin (blue) was utilized for nuclear staining. Scale bars are 100 μm.
From: Recent Evidence of the Role of CD4+ T Cell Subsets in IgG4-related Disease
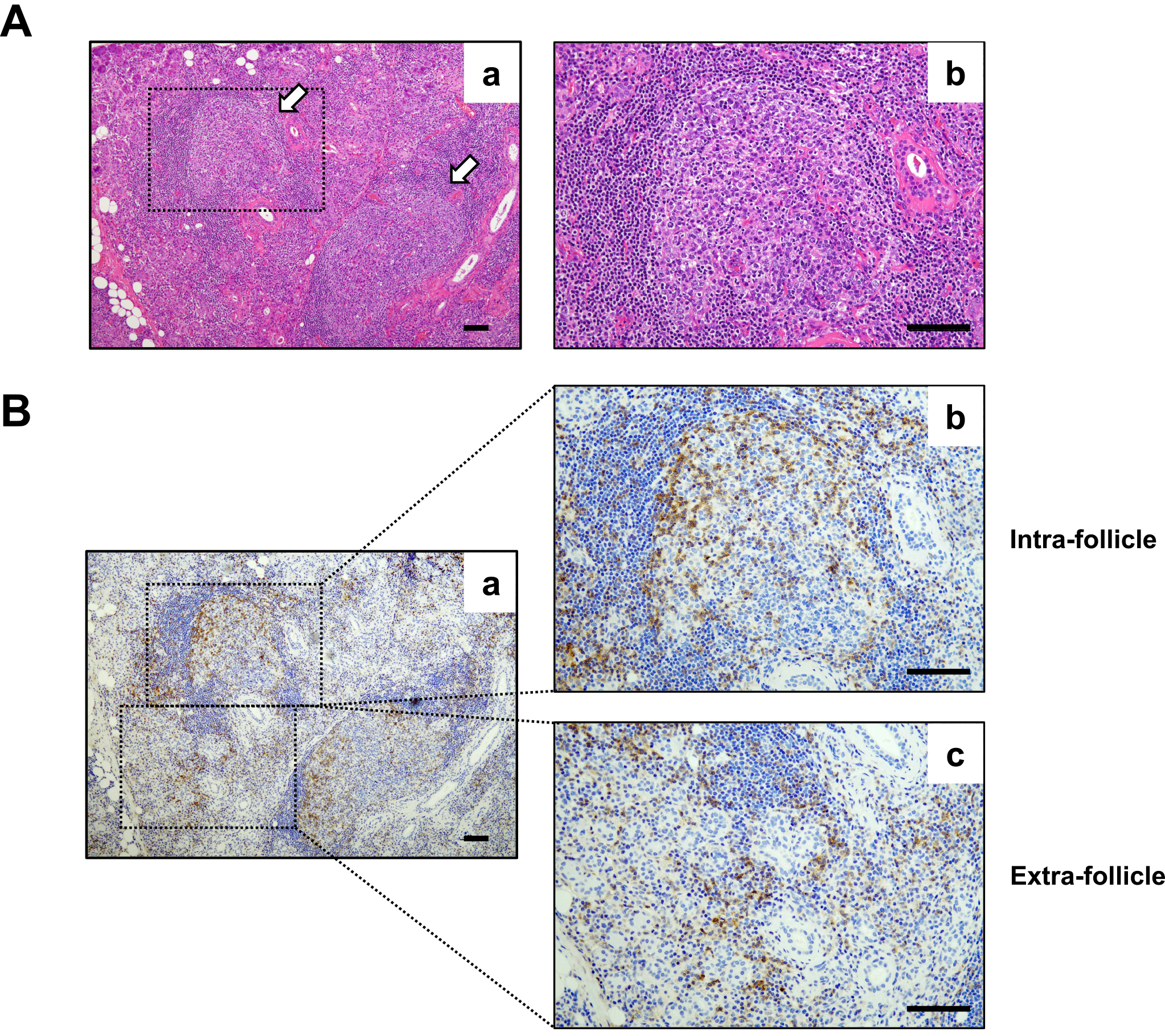
Figure 2. A model for the functional roles of PD-1hiCXCR5− T peripheral helper (Tph) cells and extrafollicular B cells in affected organs of IgG4-RD.
Tph cells accumulate in the inflamed tissues and produce factors associated with B-cell help, including IL-21 and CXCL13, which is a ligand of CXCR5. Therefore, it is believed that Tph cells can recruit B cells and Tfh cells, leading to the formation of ectopic lymphoid structures in nonlymphoid tissues. Tph cells lack CXCR5 expression and express a lower level of Bcl-6. Therefore, they are localized outside ELSs and exert their functions as B cell helpers. Tph cells may interact with extrafollicular follicular B cells (CD11c+CD21− cells, referred to as age-associated B cells, ABCs) that also lack CXCR5 expression. From our recent observations, Tph cells interact with extrafollicular B cells in affected tissues of IgG4-RD. Additionally, CD11c+CD21− B cells in IgG4-RD are a main producer of IgG4. Tph cells interact with CD11c+CD21− B cells in extrafollicles, and IL-10 produced by Tph cells may induce CSR to IgG4 in CD11c+CD21− B cells. Conversely, CD11c+CD21− B cells may influence cell growth, proliferation, and differentiation of Tph cells as antigen-presenting cells.
From: Recent Evidence of the Role of CD4+ T Cell Subsets in IgG4-related Disease