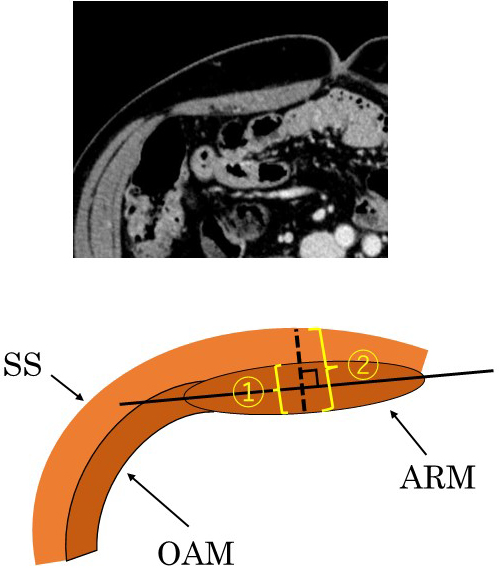
Figure 3. A. The angle between the ileostomy and the AIW is defined as the inner angle between the long axis of the abdominal rectus muscle and the straight line passing through two midpoints of the proximal lumen (at the skin and peritoneum level) (red area). All measurements are made using an axial computed tomography view.
SS, skin and subcutaneous; ARM, abdominal rectus muscle; OAM, external/internal oblique and abdominal transverse muscles; SO, stoma outlet
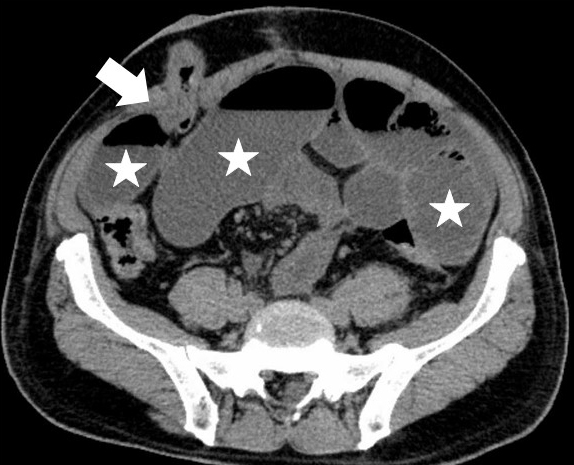
B. A CT for a patient who developed SOO. The CT findings show the proximal lumen inclines to the medial side.
White arrow heads: stoma outlet, ☆: dilated intestines.
From: Risk Factors for Stoma Outlet Obstruction: Preventing This Complication after Construction of Diverting Ileostomy during Laparoscopic Colorectal Surgery
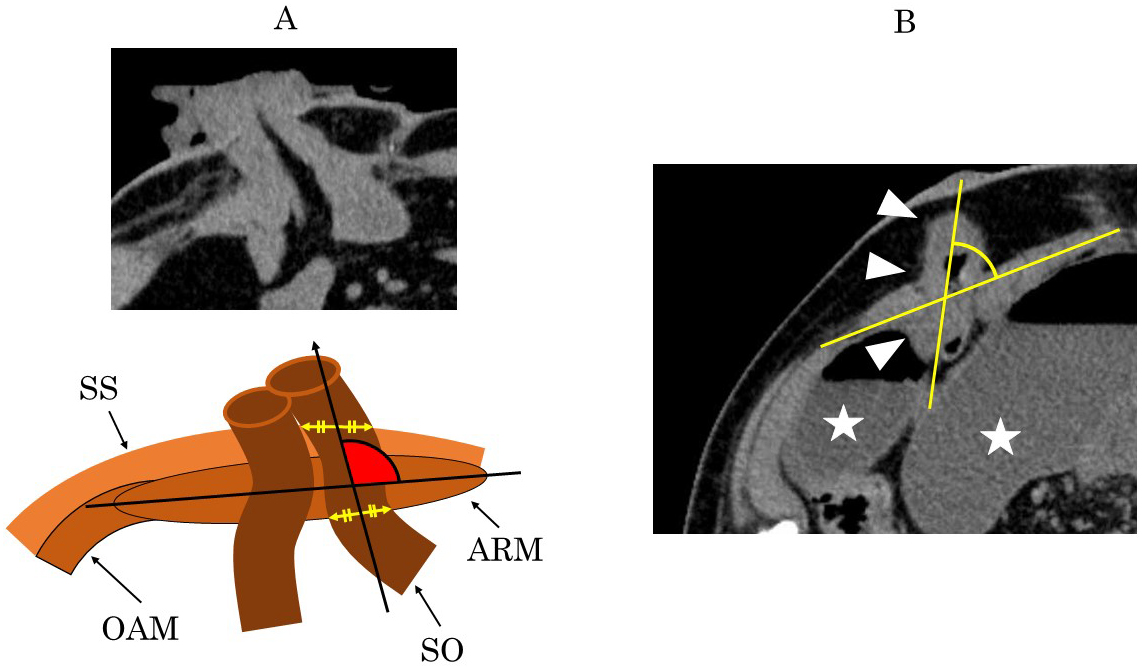
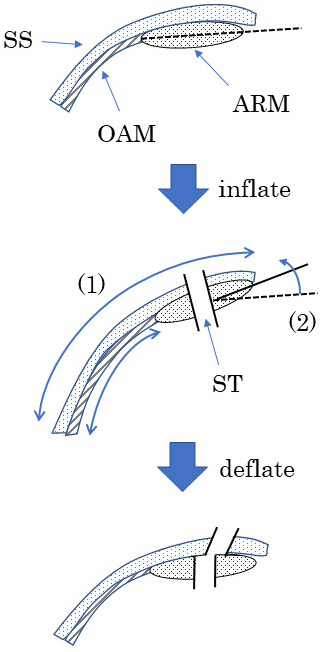
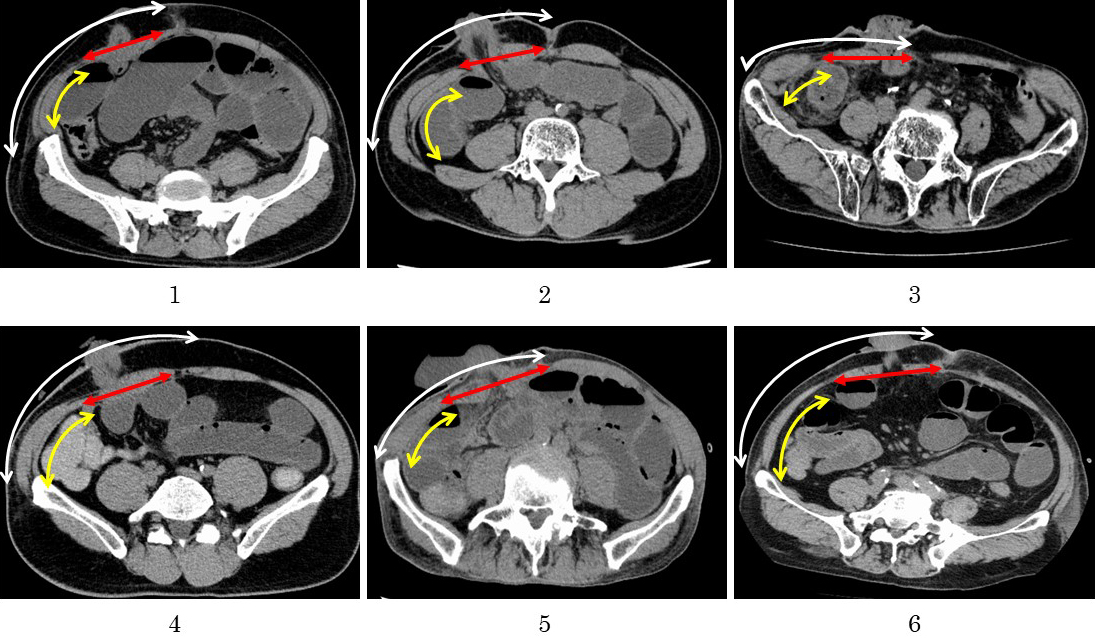
Figure 6. Two changes occur in the abdominal wall during pneumoperitoneum. (1) Due to the structural nature of the muscle fibers, the transverse abdominal muscle and the internal and external oblique muscles can extend laterally, but the abdominal rectus muscle cannot; thus, the skin and subcutaneous layer are displaced laterally from the muscular layer. (2) The angle between the long axis of the abdominal rectus muscle and the horizontal axis is increased. Due to these changes, the angle of the ileostomy outlet might tilt inward when the ileostomy is constructed under pneumoperitoneum.
SS, skin and subcutaneous; ARM, abdominal rectus muscle; OAM, external/internal oblique and abdominal transverse muscle; ST, stoma trephine.
From: Risk Factors for Stoma Outlet Obstruction: Preventing This Complication after Construction of Diverting Ileostomy during Laparoscopic Colorectal Surgery