Figure 2. Gel electrophoresis of serum in AIP reveals β-γ globulin bridging. (From Tan to Sui 22;603–608:2001 in a Japanese publication. Reprinted with permission from Igakutosho-Shuppan, Ltd.)
From: Immunoglobulin G4-related Disease: An Overview
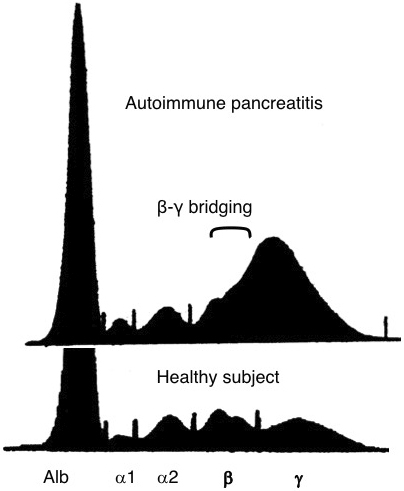
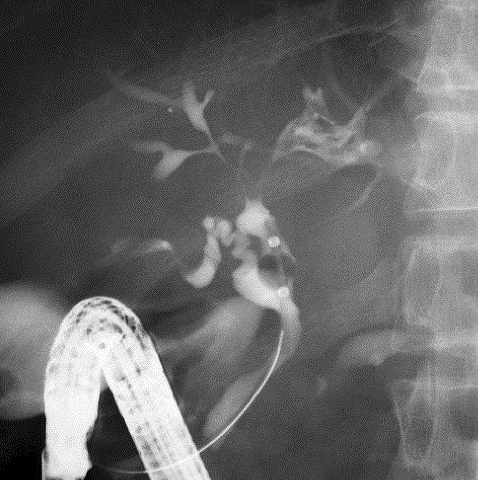
Figure 6. Image findings of AIP. (a) Endoscopic retrograde cholangiopancreatography (ERCP) typically shows characteristic irregular narrowing of the main pancreatic duct and narrowing of the lower bile duct (arrow). (b) Contrast-enhanced CT reveals a swollen pancreas with a straight margin and capsule-like, low-density rim (arrows). (From Shindan to Chiryo 104;453–458:2016 in a Japanese publication. Reprinted with permission from Igakutosho-shuppan, Ltd.)
From: Immunoglobulin G4-related Disease: An Overview
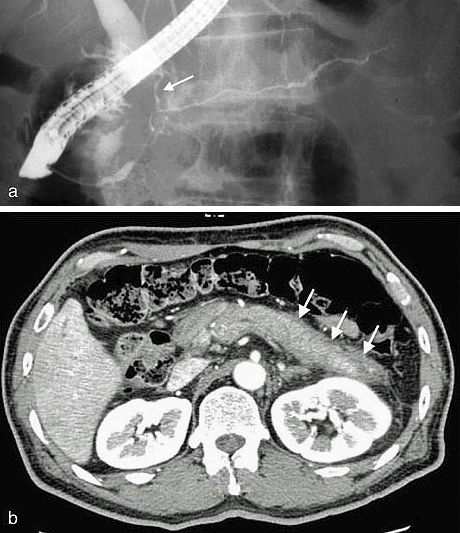
Figure 8. Image findings of a 72-year-old man with focal AIP. (a) Contrast-enhanced CT disclosed a localized attenuated mass at the pancreatic body (circle). (b) EUS showed a low-echo pancreatic mass with high-echo spots (arrow). (c) Contrast-enhanced CT revealed left kidney involvement with renal cortical lesions of decreased enhancement (circle). (d) Contrast-enhanced CT showed a soft tissue mass around the abdominal aorta (arrow).
From: Immunoglobulin G4-related Disease: An Overview
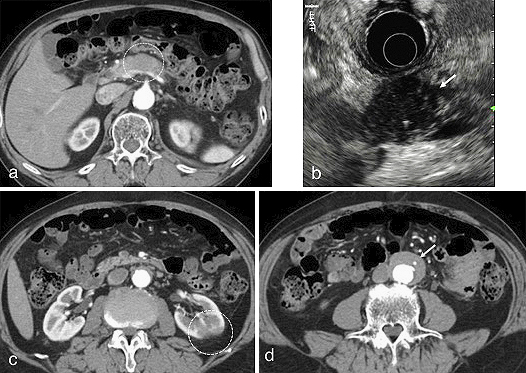
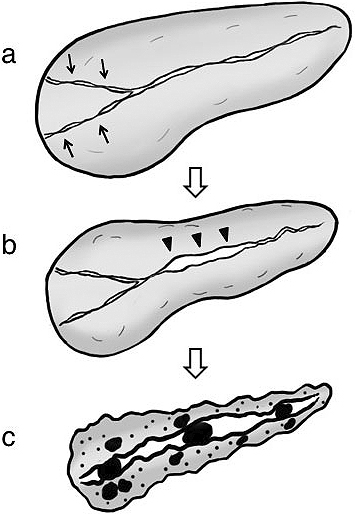
Figure 9. Sequential progression mechanism of AIP to confirmed chronic pancreatitis. (a) Narrowing of both Wirsung’s and Santorini’s ducts (arrows) by pancreatic head swelling causes pancreatic juice stasis in the upstream pancreatic duct. (b) Pancreatic juice stasis results in increased intrapancreatic duct pressure that is resistant to typical AIP-specific main pancreatic duct narrowing in the pancreatic body region, leading to ductal nonnarrowing in this region (arrowheads). (c) In concert with relapse, these events ultimately result in severe calcification. (From Ref. 51. Reprinted with permission.)
From: Immunoglobulin G4-related Disease: An Overview