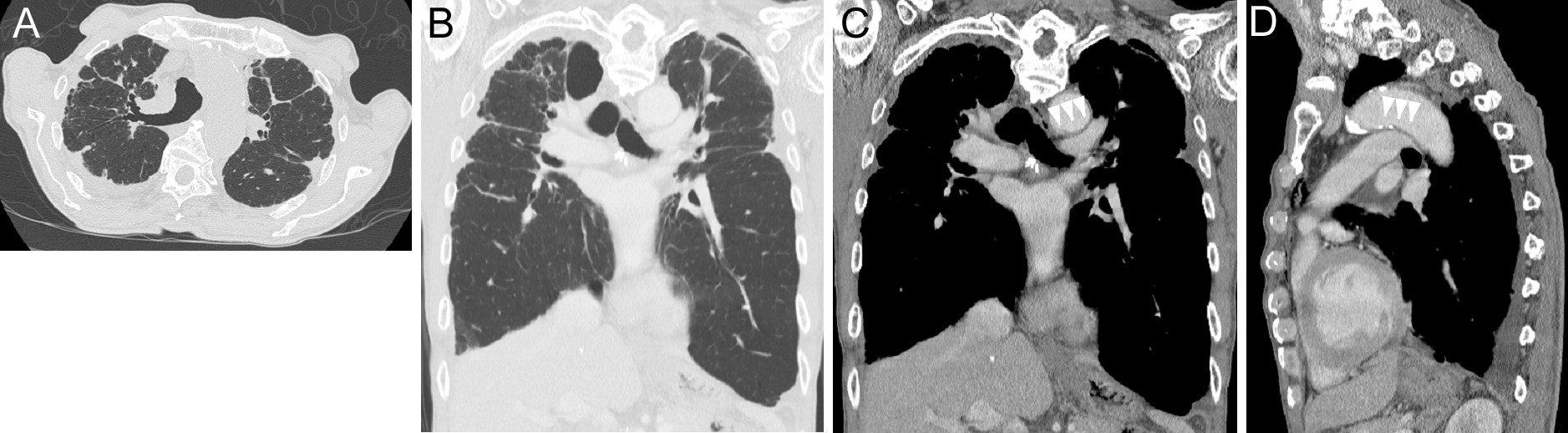
Figure 2. CT of the chest, showing bilateral subpleural predominant consolidation with traction bronchiectasis and volume loss. The lesion was predominant in the right lung, and cysts and traction bronchiectasis were widely observed in the right upper lobe. The volume loss of the right upper lobe was remarkable, and a rightward mediastinal shift was noted (A, transverse view of high-resolution CT on initial consultation; B, coronal view responding to C at the onset of hoarseness 2 months after the initial consultation). The aortic arch and left pulmonary artery were closely contacted, possibly compressing the left recurrent laryngeal nerve (white arrowheads in C, coronal view, and in D, sagittal view at the onset of hoarseness).
From: Left Vocal Cord Paralysis in Idiopathic Pleuroparenchymal Fibroelastosis: A Case Report