Corresponding author: Eisuke Adachi, eadachi-ims@umin.ac.jp
DOI: 10.31662/jmaj.2018-0025
Received: August 20, 2018
Accepted: December 12, 2018
Advance Publication: February 1, 2019
Published: March 4, 2019
Cite this article as:
Adachi E, Koibuchi T, Yotsuyanagi H. Gastric Syphilis in a Human Immunodeficiency Virus–Infected Patient. JMA J. 2019;2(1):93-94.
Key words: Gastric syphilis, unusual complications of syphilis, Immunostaining, Human immunodeficiency virus
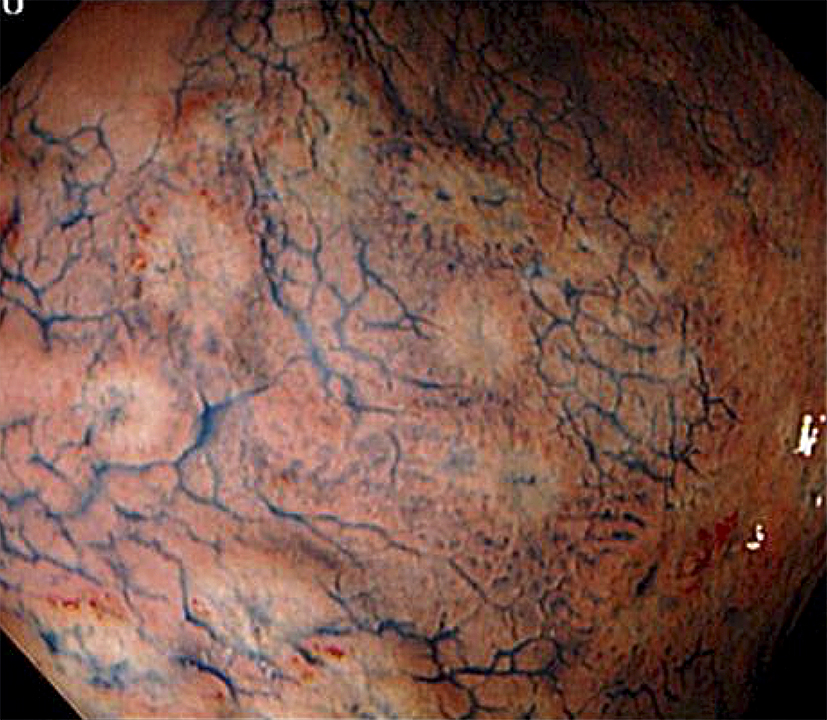
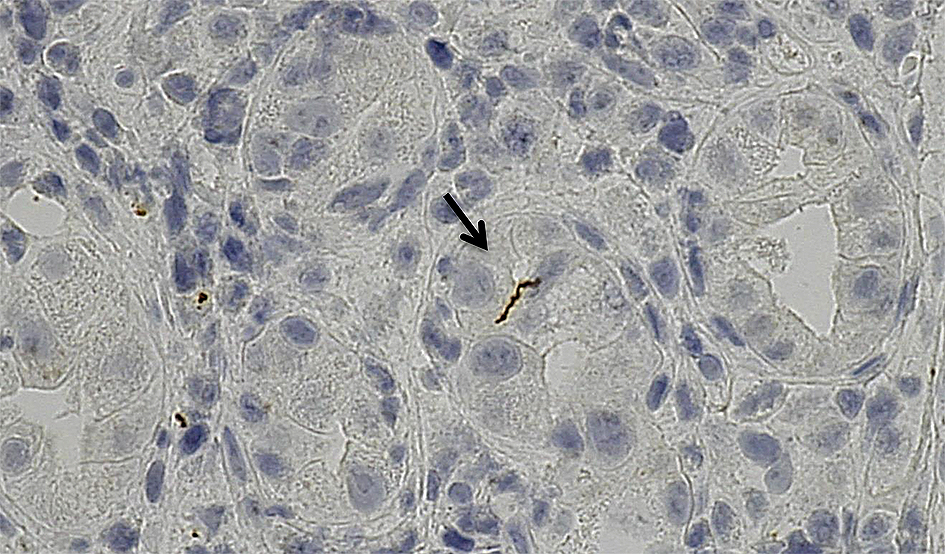
A 35-year-old homosexual man with HIV receiving antiretroviral therapy was admitted to our hospital because of epigastric discomfort that developed three weeks earlier. There were no lesions inside his genital area and no characteristic rash of syphilis. However, gastroduodenoscopy revealed diffuse erosive lesions in the gastric mucosa (Figure 1) and spirochete cells were identified by immunostaining the biopsy specimens (Figure 2). He was diagnosed with syphilis on the basis of the serological test for syphilis. The gastric lesions disappeared after the administration of amoxicillin. We infer that the gastric syphilis was caused by hematogenous dissemination. Some reports have described that intestinal complications are seen in persons who have anal intercourse (1). Syphilis is a forgotten etiology of active gastritis (2). Gastric syphilis has become less common, owing to the advances in techniques for the early diagnosis and treatment of syphilis. Immunostaining with anti-Treponema pallidum antibodies helps in histologically identifying Treponema pallidum.
None
This work was supported by JSPS KAKENHI grant number 17K16222.
EA carried out this work and drafted the manuscript. EA, KT, and HY designed the project and revised the manuscript.
A written informed consent was obtained from the patient.
This work was approved by the Institutional Review Board The Institute of Medical Science, The University of Tokyo (accession number:18-11-1003)
