Corresponding author: Tetsuya Hashimoto, tetsuyahashimoto629@hotmail.co.jp
DOI: 10.31662/jmaj.2022-0169
Received: August 31, 2022
Accepted: September 26, 2022
Advance Publication: November 30, 2022
Published: January 16, 2023
Cite this article as:
Hashimoto T, Matsuyoshi A, Shiraishi W. Migration of Vasoconstriction in Reversible Cerebral Vasoconstriction Syndrome. JMA J. 2023;6(1):88-89.
Key words: Magnetic resonance imaging, reversible cerebral vasoconstriction syndrome, thunderclap headache
A 49-year-old woman developed thunderclap headaches triggered by straining during defecation. Magnetic resonance imaging (MRI) on day 3 after the onset revealed somewhat poor delineation of the bilateral distal posterior cerebral arteries without cerebral parenchymal lesions, which suggested possible vasoconstriction (Figure 1A and 1B). There were no intra-arterial signals on fluid-attenuated inversion recovery images and thereafter headaches during defecation remained. On day 17, although the visualization of the posterior cerebral arteries was improved, the basilar artery showed segmental constriction (Figure 1C). Basi-parallel anatomical scanning revealed segmental constriction of the external vessel wall of the basilar artery (Figure 1D). Reversible cerebral vasoconstriction syndrome (RCVS) was diagnosed and verapamil was administered. The patient’s headaches gradually disappeared and vasoconstriction was resolved on MRI on day 31.
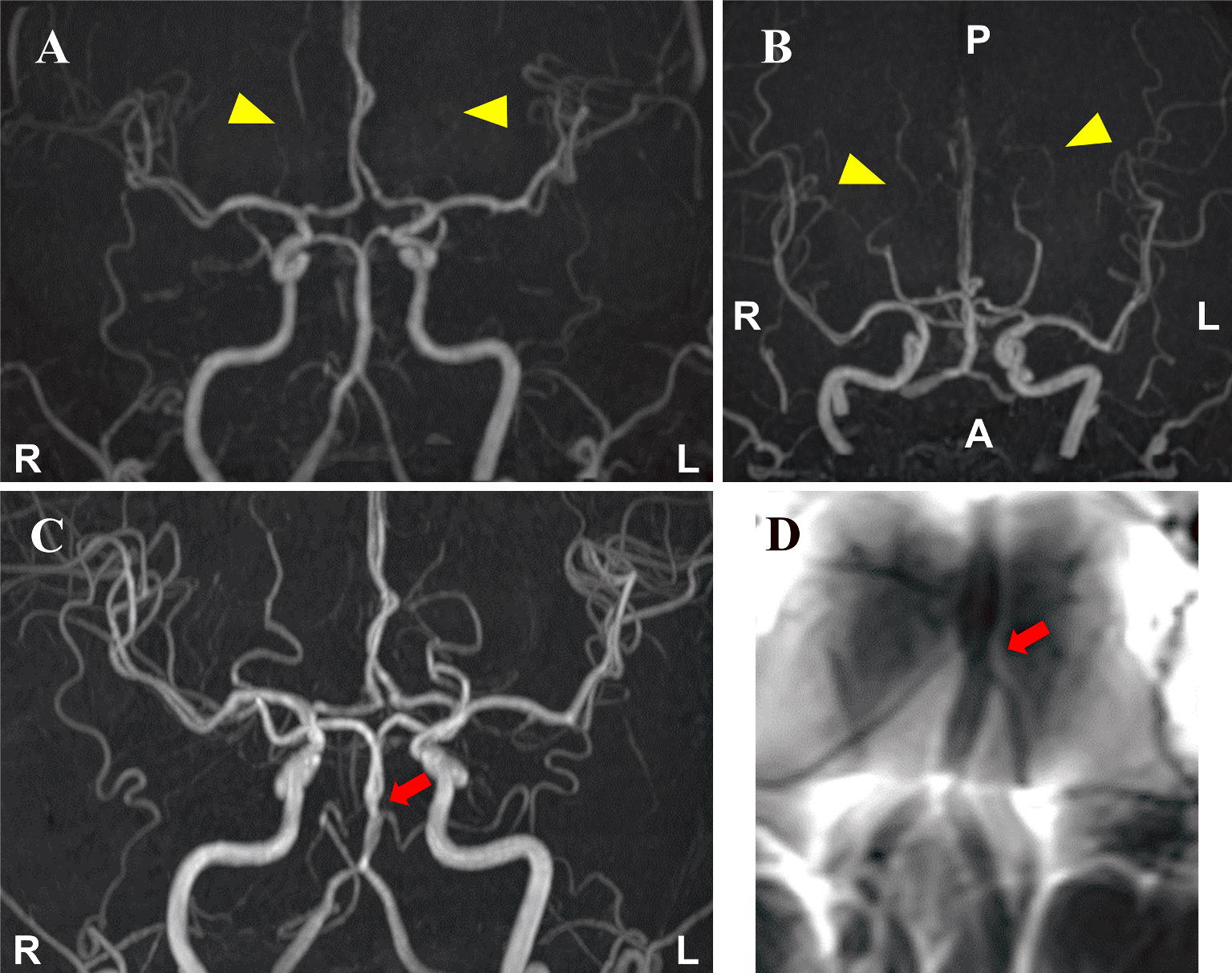
In RCVS, vasoconstriction can be difficult to detect in very distal branches, which can make its diagnosis challenging (1). Vasoconstriction has been reported to start at distal vessels and migrate more proximally to larger vessels (2). Therefore, serial MRI examinations are important for diagnosing RCVS.
None
All authors contributed to patient care. Tetsuya Hashimoto wrote the manuscript and the other authors revised it.
This study did not require IRB approval.
Written informed consent was obtained from the patient to publish.
Ducros A, Boukobza M, Porcher R, et al. The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome. A prospective series of 67 patients. Brain. 2007;130(12):3091-101.
Shimoda M, Oda S, Hirayama A, et al. Centripetal propagation of vasoconstriction at the time of headache resolution in patients with reversible cerebral vasoconstriction syndrome. AJNR Am J Neuroradiol. 2016;37(9):1594-8.
