Corresponding author: Daisuke Nishioka, daisuke.nishioka@ompu.ac.jp
DOI: 10.31662/jmaj.2024-0062
Received: April 1, 2024
Accepted: April 9, 2024
Advance Publication: June 28, 2024
Published: July 16, 2024
Cite this article as:
Kawachi H, Nishioka D. Health Statuses of People in Poverty Receiving Public Assistance in Japan: A Scoping Review. JMA J. 2024;7(3):301-312.
Background: Promoting health and well-being is essential to ensure dignified lives of the entire population, including those living in poverty. Guaranteeing the human right to health is a critical responsibility of social security policies. To address emerging issues associated with poverty, the Japanese government has implemented a welfare program known as public assistance―seikatsu-hogo. However, financial welfare programs may not fully mitigate health risks due to the complex impact of poverty on health. Although a global systematic review of the health status of public and social assistance recipients has been conducted, it did not include any studies from Japan. Furthermore, evidence for the development of health support strategies for Japanese recipients remains scarce. This scoping review aims to identify the current situation and potential issues concerning the health of recipients.
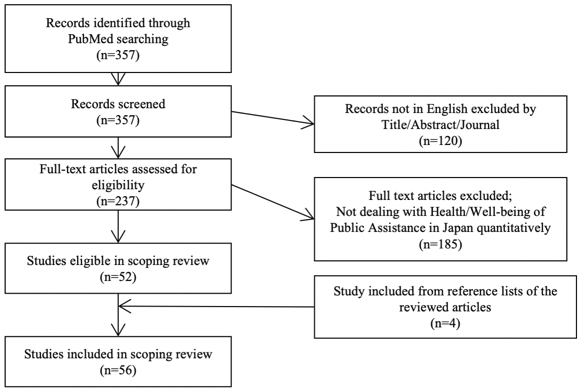
Methods: PubMed was searched for articles published before November 2023. Of the 357 articles identified, 56 were included. Among those included, 35 used the individual status of receiving public assistance as an exposure variable, 13 considered public assistance recipients as the study population, and 8 used the prefectural proportion of the population receiving public assistance as an environmental predictor.
Results: We found that public assistance recipients tend to have more disadvantageous health and well-being statuses than the general population, as reported in the global systematic review. Health inequalities were also observed among recipients based on their sociodemographic characteristics. In Japan, public assistance recipients face several health risks and are at a disadvantage compared with the general population.
Conclusions: The distribution of risks is heterogeneous among recipients, despite the minimum income protection and financial benefits in health and long-term care use. Further studies to identify the effects of public assistance policy on the health of the impoverished population, evidence-based discussions, and reform of social security policies are warranted.
Key words: Poverty, Public assistance, Scoping review, Japan
Promoting health and well-being are prerequisites for the dignified lives of the entire population, and guaranteeing the human right to health for the people is one of the important roles and responsibilities of society and social security policies (1), (2), (3). However, global evidence has recently indicated that people’s social backgrounds and contexts certainly inhibit their health-promoting activities and healthy lifestyles, resulting in health inequalities across their socioeconomic statuses (4), (5). Poverty is known to be a major, but unmet, social determinant of health. People living in poverty have insufficient resources to meet their health needs, which can impede cognitive function, resulting in difficulty making reasonable health investments and leading to adverse health outcomes (6), (7). Thus, it is imperative to reform the social security system to address the negative health effects of poverty.
In recent decades, Japan has been facing emerging issues associated with poverty. For example, Japan’s poverty rate was reported to be 15.4% in 2021, which is higher than the average among member nations of the Organization for Economic Cooperation and Development (8). In particular, the poverty rate among children living with single parents has been raised as a serious problem. Approximately half of children living with single parents live below the poverty line. The Constitution of Japan Article 25 stipulates that “All people shall have the right to maintain the minimum standards of wholesome and cultured living” and that “In all spheres of life, the state shall use its endeavors for the promotion and extension of social welfare, security, and public health (9).” As a measure to embody this clause, a governmental welfare program called public assistance―seikatsu-hogo―exists, which can benefit households living below the poverty line. The Municipal Welfare Office conducts rigorous means tests and determines whether people will receive benefits (10). Approximately 1.6% of the entire population in Japan was receiving public assistance in 2021. Households receiving public assistance can benefit from monthly minimum income benefits and are fully exempt from payments for healthcare and long-term care utilization (10).
Considering the potential influence of multidimensional poverty (11), financial welfare programs may not fully compensate for socioeconomic health risks. A previous review by Shahidi et al. reported that the health status of public and social assistance recipients in high-income countries is not better than that of nonrecipients (12). From the review, public or social assistance recipients have poorer subjective health; a higher prevalence of mental illness, including anxiety and depression, diabetes, and obesity; and a higher mortality rate than the general population not receiving public or social assistance. Furthermore, public and social assistance recipients have been reported to be more likely than nonrecipients to engage in high-risk health behaviors, such as smoking, problematic drinking, and frequent visits to healthcare institutions. Shahidi et al. summarized these findings and suggested that public and social assistance programs may not sufficiently protect the health of recipients.
Since the fiscal year 2021, from the perspectives of promoting health and optimizing medical assistance costs for public assistance recipients, a health support program for public assistance recipients―kenko-kanri-shien-jigyo―has been mandated in municipal offices. This program emphasized the importance of a data-driven approach. However, because public and social assistance systems vary across countries and the review by Shahidi et al. did not include any Japanese evidence (12), the generalizability of the evidence was unclear. In addition, quantitative data on health support strategies for recipients of public assistance in Japan remain sparse. Summarizing the existing evidence to develop evidence-based health support policies for recipients is urgently needed.
In this study, we aimed to conduct a literature review of existing peer-reviewed research that has dealt with the health and health behaviors of public assistance recipients in Japan. Considering the findings of this review, we further aimed to organize the evidence and summarize emerging issues that can contribute to the discussion of effective interventions to support health among recipients.
A scoping review.
We used the population, concept, and context framework to define the inclusion criteria. All published studies using public assistance recipients in Japan, both as an exposure variable and study population, were eligible. We reviewed the existing literature describing the health and well-being of public assistance recipients as an outcome measure. We restricted our search to English-language and peer-reviewed publications. We excluded gray literature, working papers, and peer-reviewed commentaries lacking direct empirical tests.
We conducted a search on PubMed using the term ((“public assistance” [MESH] or “public assistance”) AND (Japan)) on November 7, 2023. We supplemented our electronic search by searching the reference lists of all the included literature and related review articles.
The studies were independently selected by two researchers (HK and DN). The two researchers compared their lists, and any differences in opinions were resolved through discussion.
Data were extracted by the authors using standard data extraction forms, including the PMID, title, author names, and publication year of the articles. Whether public assistance was used as an exposure variable or as a study population was coded. If a study utilized public assistance as an exposure variable, we extracted the study design, setting, reference group information, study participants, sample size, study outcomes, and study findings. If the study utilized public assistance recipients as the entire study population, the study design, setting, sample size, and findings were extracted.
A total of 357 articles were identified in the search, of which 52 met the eligibility criteria of this review (13), (14), (15), (16), (17), (18), (19), (20), (21), (22), (23), (24), (25), (26), (27), (28), (29), (30), (31), (32), (33), (34), (35), (36), (37), (38), (40), (41), (42), (43), (44), (45), (46), (47), (48), (49), (50), (51), (52), (53), (54), (55), (56), (57), (58), (59), (60), (61), (62), (63), (64). From the review, four eligible studies were additionally included (65), (66), (67), (68). Finally, 56 articles were included. The selection process of the study is illustrated in Figure 1. There have been no randomized controlled trials on this study design.
A total of 35 studies utilized public assistance status as the exposure variable (13), (14), (15), (16), (17), (18), (19), (20), (21), (22), (23), (24), (25), (26), (27), (28), (29), (30), (31), (32), (33), (34), (35), (36), (37), (38), (39), (40), (41), (42), (43), (44), (65), (66), (67). Among them, seven used public data obtained from national or local governments (17), (21), (22), (23), (27), (32), (38). One study used registry data obtained from medical institutes (35). Majority of the studies used data collected from medical records and/or administered surveys through questionnaires or interviews with healthcare providers at medical institutes. A higher mortality (67), prevalence of infections (24), chronic diseases (diabetes complications (19), (36) and heart diseases (30), (31), (35)), and adverse health outcomes of surgeries (15) were observed. Unpreferable health behaviors were also prevalent among public assistance recipients such as smoking (31), frequent medical visits (25), (26), (38), (65), polypharmacy (40), (41), less vaccine uptake (42), and refraining from necessary healthcare-seeking behaviors (16), (27), (44). However, several studies have also demonstrated an association or no association between receiving public assistance and favorable health outcomes/behaviors (14), (17), (18), (28), (32), (34). In a multicenter prospective cohort study, Kaneko et al. investigated that the receipt of public assistance was inversely associated with all-cause mortality among patients who had started receiving regular physician-led health care at home or at nursing homes (28). Furthermore, among patients who were diagnosed with methamphetamine use disorder, those who received public assistance were more likely to remain in treatment at 3 months than those who did not (Table 1) (14).
Table 1. Descriptive Information of the Studies Using Public Assistance as an Exposure Variable.
| Authors | Year | Study design | Setting/participants | Data | Reference group | N (public assistance (PA)/non-PA) |
Outcome | Findings |
|---|---|---|---|---|---|---|---|---|
| Noda T, et al. (13) | 2001 | Prospective cohort study | Patients with alcoholism attending to an abstinence self-help group | Medical records and a follow-up interview with each patient or their family | Nonrecipients | 306 (83/214), 9 had no information on receiving PA | Stable abstinence from alcohol and mortality | Non-PA recipients have more preferable odds of stable abstinence from alcohol (OR: 7.2, 95% CI: 1.8-28.4) and lower mortality (HR: 0.5, 95% CI: 0.4-0.8) than PA recipients |
| Kobayashi O, et al. (14) | 2008 | Case-control study | Single center/patients diagnosed with methamphetamine use disorder (aged 19-60 years) | Medical records | Nonrecipients | 101 (26/75) | 3-month treatment retention | The treatment retention group had a significantly larger proportion of patients receiving PA (38% vs. 17%). Those who received PA were twice as likely to remain in treatment as those without, although the p-value was statistically borderline (adjusted OR: 2.38, 95% CI: 0.92-6.16, p = 0.074) |
| Wada T, et al. (15) | 2009 | Retrospective cohort study | Patients with lateral epicondylitis treated with arthroscopic surgery (aged 42-71 years) | Medical records and a self-administered questionnaire survey | Nonrecipients | 18 (4/14) | Disability of the Arm, Shoulder, and Hand score | PA was found to be a potential predictor of a poorer outcome after arthroscopic surgery for lateral epicondylitis (median score: 36.5 vs. 2.2, p = 0.03) |
| Kamimura A, et al. (16) | 2013 | Retrospective cohort study | Data were collected through semistructured, in-person interviews with women who had experienced any type of intimate partner violence (IPV) in their lives (aged 24-80 years) | Interview survey | Nonrecipients | 3,403 person-years of 101 respondents, including 154 person-years of the recipients | Intimate partner violence-specific healthcare-seeking behavior | Receiving PA was associated with IPV-specific healthcare-seeking behavior (coef.: 1.08, SE: 0.48) |
| Uchimura K, et al. (17) | 2015 | Retrospective cohort study | Newly registered tuberculosis (TB) patients aged 15-59 years in Japan | Nationally representative registry data | Other insurance | 9,097 (711/uninsured: 321, insured: 8,065) | Tuberculosis death | The association between PA and death from tuberculosis disappeared in the multivariate model. However, the association remained among the uninsured (aHR [95% CI]: 1.08 [0.78-1.51] and 1.48 [1.02-2.15], for PA and uninsured, respectively). PA, particularly if limited to casual workers and unemployed persons, may contribute to the improvement of survival rates (from the Kaplan-Meier curve results) |
| Takenaka Y, et al. (18) | 2016 | Retrospective cohort study | Single center/newly diagnosed and histologically confirmed patients with head and neck squamous cell carcinoma (HNSCC), median age 76 years (range 28-92) | Medical records | Other insurance | 407 (72/335) | Mortality | The clinical stage distribution was not significantly different between the PA groups and other insurances (OR: 1.36, 95% CI: 0.78-2.39, for stages III and IV). The 5-year overall survival, cumulative incidence of HNSCC death, and cumulative incidence of other death rates were 63.3% and 59.1%, 27.0% and 31.8%, and 10.3% and 9.7% for the PA and other insurance groups, respectively. The adjusted subdistribution HR for the association between PA and HNSCC death was 0.73 (95% CI: 0.44-1.21) |
| Funakoshi M, et al. (19) | 2017 | Cross-sectional study | Multicenter/young adult patients (aged 20-40 years) with type 2 diabetes (T2DM) | Medical records and a self-administered questionnaire survey | Other insurance | 672 (64/608) | Diabetic complication | PA recipients have a higher odds ratio of having diabetes complications after adjusting for general risk factors (an OR of 2.19 (1.20-3.95) for retinopathy and an OR of 2.60 (1.16-5.50) for nephropathy |
| Kawahara YY, et al. (20) | 2017 | Retrospective cohort study | Single center/patients admitted to the emergency room and then had an episode of self-harm | Medical records | Nonrecipients | 405 (54/351) | Repetition of short-term self-harm (<1 month and <6 months) | Living on PA was associated with repetition of self-harm within 6 months (multivariable HR: 3.126 [1.699-5.754]). |
| Nakanishi M, et al. (21) | 2017 | Panel data | National Patient Survey | Nationally representative survey data | Nonrecipients | 13,014 (1,112/11,902) | Deliberate self-harm | The proportion of patients receiving PA was higher in those who had engaged in deliberate self-harm (8.5%) than in the general population |
| Yuda M. (22) | 2018 | Cross-sectional study | - The Fact-Finding Survey on Medical Assistance (Iryo-Fujo Jittai Chosa). - The Survey of Medical Care Activities in Public Health Insurance (Syakai Iryo Shinryo-Koui Betsu Chosa) |
Nationally representative sets of individual-level claims data | Other insurance | 299,520 (18,693/280,827) | Inpatient care elasticity | The medical expenditure is significantly higher for medical assistance patients than for other medical health insurance patients, with an arc elasticity of approximately 0.20 |
| Izumi K, et al. (23) | 2019 | Panel data | One municipality/patients with culture-positive TB notified with genotype data of Mycobacterium tuberculosis | Registry data | Nonrecipients | 1,025 (304/720), 1 had no information on receiving PA | Clustered cases | Receiving PA (adjusted OR: 1.81, 95% CI: 1.15-2.84) at the time of tuberculosis diagnosis was associated with genotype clustering |
| Cho T, et al. (24) | 2020 | Retrospective cohort study | Single center/women who underwent Chlamydia trachomatis testing during a singleton pregnancy and delivered after the 22nd week of gestation (control group: randomly selected individuals from among patients with negative results) | Medical records | Nonrecipients | 2,233 (74/2,159) | Preterm birth | The Chlamydia-positive group had a higher rate of PA coverage than the control group (12.4% vs. 2.1%) |
| Ikeda K, et al. (65) | 2020 | Case-control study | Single center/patients who visited the Emergency Department (ED), aged ≥20 years | Medical records | Other insurance | 340 (27/313) | Frequent ED use | The receipt of PA significantly increased the OR for frequent visits even after adjusting for sex, age, and potential confounding factors (OR: 3.89, 95% CI: 1.62-9.35) |
| Kaneko M, et al. (25) | 2020 | Cross-sectional study | Multicenter/patients who presented to the EDs | Medical records | Nonrecipients | 20,388 (110/20,257), 21 had no information on receiving PA | Frequent ED use | Receiving PA (adjusted OR: 7.19, 95% CI: 2.87-18.07) had an association with frequent ED visits |
| Osawa I, et al. (26) | 2020 | Cross-sectional study | Single center/ED patients (age ≥ 18 years) | Medical records | Nonrecipients | 556 (37/519) | Hospitalization rates | Frequent ED users tended to receive PA more than nonfrequent ED users (8.9% vs. 4.7%). The risk for hospitalization was not associated with frequent ED use (adjusted OR: 1.21, 95% CI, 0.74-1.96) |
| Yoshikawa R, et al. (27) | 2020 | Panel data | Japanese tuberculosis surveillance data | Registry data | Other insurance | 88,351 (7,148/81,203) | Patient delay (the time from the onset of symptoms to the initial doctor visit): short, moderate, and long delay | Receiving PA was specifically a risk factor for moderate and long delays (adjusted OR [95% CI]: 1.19 [1.09-1.31] and 1.36 [1.16-1.60] for moderate and long delays, respectively) |
| Kaneko M, et al. (28) | 2021 | Prospective cohort study | Multicenter/patients who had started receiving regular physician-led health care at home or at nursing homes, aged ≥65 years | Survey data, administered by physicians | Nonrecipients | 825 (115/710) | All-cause mortality | A multivariate Cox proportional-hazards model showed that nonreceipt of PA was associated with mortality, indicating that patients who received PA were less likely to die, adjusted HR: 0.61 (0.41-0.90) with multiple imputation (complete case analysis, n = 663: 0.65 [0.42-1.01]) |
| Koyama Y, et al. (29) | 2021 | Cross-sectional study | One municipality/a survey was administered to caregivers of all 6-7-year-old children attending public elementary schools | Social survey data (self-questionnaire) | Low-income (LI) households without PA | 6,920 (PA(+)/LI(+): 191, PA(−)/LI(+): 452, PA(−)/LI(+): 6,277) | Child mental health assessed using the Strength and Difficulties Questionnaire (SDQ) and child resilience assessed using the Children’s Resilient Coping Scale (CRCS) |
The SDQ and CRCS scores were not significantly different between recipients or nonrecipients of PA. However, the mental health outcomes were worse in PA recipients across all scores, particularly emotional symptoms and prosocial behavior. Children in households receiving PA had a higher risk of school refusal than those in households not receiving PA; children living in PA household were four times more likely to refuse to go to school than children living in LI households without PA (OR: 4.00, 95% CI: 0.85-18.84, p = 0.080) |
| Watanabe S, et al. (30) | 2021 | Retrospective cohort study | Single center/patients with ST-segment elevation myocardial infarction | Medical records | Nonrecipients | 525 (67/458) | Clinical features | The prevalence of smoking was higher in the PA group than in the non-PA group (91.0 vs. 81.1%, p = 0.02). The high-density lipoprotein cholesterol level in the PA group was lower than that in the non-PA group (43.2 ± 9.9 mg/dL vs. 47.1± 12.8 mg/dL, p = 0.005). Ventricular arrhythmia on admission was significantly more frequent in the PA group than in the non-PA group (11.9 vs. 4.8%, p = 0.02). The left ventricular ejection fraction in the PA group was lower than that in the non-PA group (in the acute phase 46.6% ± 10.7 vs. 53.3± 8.6, p = 0.001; in the chronic phase 48.7% ± 10.1 vs. 55.3 ± 9.4, p = 0.008) |
| Fujito H, et al. (31) | 2022 | Retrospective cohort study | Single center/patients who were admitted for acute heart failure (HF) and were discharged or transferred to another hospital, followed up for 1 year | Medical records | Other insurance | 771 (87/684) | Cardiac events (death from cardiovascular disease (CVD) or readmission) after discharge | The PA group was significantly younger and had a higher incidence of diabetes, smoking, and ischemic and hypertensive heart disease as well as lower estimated glomerular filtration rate than the non-PA group (all P < 0.05). Patients with acute HF covered by PA received the same quality of medical care, including invasive therapy, as those not covered by PA After adjusting for covariates, PA was independently associated with 1-year cardiac event rate (HR: 2.15, 95% CI: 1.42-3.26) |
| Kaneko M, et al. (32) | 2022 | Cross-sectional study | One municipality/older adults aged 75 years or older who visited medical facilities at least four times a year | Claims data | Nonrecipients | 413,600 (14,243/399,357) | Care fragmentation (Fragmentation of Care Index (FCI)) | Multivariable analysis revealed that patients receiving PA had a lower FCI than those not receiving PA, with a coefficient of 0.137 (This can be explained by the fact that people receiving PA need to report to the local government the name of the medical institution where they would like to visit.) |
| Kino S, et al. (33) | 2022 | Cross-sectional study | 39 municipalities/older community-dwelling recipients | Social survey data (self-questionnaire) | Nonrecipients | 93,280 (1,093/92,187) | Depressive symptoms (Geriatrics Depression Scale GDS) | The older PA recipients have a higher prevalence of depressive symptoms (PR 1.57 [95% CI: 1.47-1.67]) than nonrecipients |
| Kino S, et al. (66) | 2022 | Cross-sectional study | 39 municipalities/older community-dwelling recipients | Social survey data (self-questionnaire) | Nonrecipients | 16,135 (202/15,933) | Suicidal ideation and attempts | PA recipients had a higher prevalence of lifetime suicidal ideation (PR: 1.47, 95% CI: 1.02-2.13) and a higher prevalence of attempted suicide (PR: 1.91, 95% CI: 1.20-3.04) than nonrecipients |
| Nakayama T, et al. (34) | 2022 | Case-control study | Single center/patients who initiated maintenance dialysis (median age (IQR) 70 (59-79) years) | Medical records | Nonrecipients | 355 (13/342) | Peritoneal dialysis (PD) selection | Multivariate analysis revealed that PA (OR: 0.70; 95% CI: 0.08-6.09, p = 0.74) was not significantly associated with PD selection |
| Nishimoto Y, et al. (35) | 2022 | Retrospective cohort study | Multicenter/patient with acute HF (AHF) and patients who were hospitalized because of AHF for the first time | Registry data | Nonrecipients | 3,728 (218/3,510) | Cumulative 1-year incidences of all causes of death, HF, and hospitalizations after discharge | The adjusted risk for HF hospitalization beyond 180 days was significant in those with PA (HR: 1.56, 95% CI: 1.07-2.29, p = 0.02) |
| Sengoku T, et al. (36) | 2022 | Cross-sectional study | People residing in Japan during the years 2015-2017 | National Database (NDB) and Medical Assistance Claims data | Nonrecipients | The total numbers of recipients in Japan during 2015, 2016, and 2017 were 2,161,442, 2,148,282, and 2,130,482, respectively | Type 2 diabetes prevalence | The mean crude prevalence and age-standardized prevalence of diabetes (inpatients and outpatients) among 47 prefectures were 7.8% in recipients and 3.9% in public health insurance enrollees. In the city-level analysis, the odds ratio for the prevalence of T2D by region ranged from 0.31 to 1.51 |
| Wakata S, et al. (37) | 2022 | Repeated cross-sectional study | Patients in a single center clinic | Clinic medical records | Nonrecipients | 374 (68/306) | The Health-Related Quality of Life by SF-12 score, with three components: physical health component summary (PCS), mental health component summary (MCS), and role-social component summary (RCS) |
The PA recipients had lower PCS and RCS scores than those not receiving any welfare benefit (PCS Beta: −8.24, 95% CI: −10.43 to −6.05; RCS Beta: −7.87, 95% CI: 11.88 to −3.85). A decline in the MCS score was observed more in PA recipients than in those not receiving any welfare benefits during the COVID-19 pandemic (Beta: −4.27, 95% CI: −6.67 to −1.82) |
| Yuda M. (38) | 2022 | Cross-sectional study | - The Fact-finding Survey on Medical Assistance for PA patients - the Survey of Medical Care Activities in Public Health Insurance for the universal public health insurance patients |
Nationally representative sets of individual-level claims data | Other insurance | 1,698,857 (261,546/1,437,311) | Outpatient care utilization | PA assignment increases monthly healthcare expenditure by approximately 20% and the monthly number of doctor visits by approximately 25%. When imposing a copayment on PA beneficiaries, monthly healthcare expenditure significantly decreases by approximately 25.0% and the number of visits by approximately 30%. The estimated price elasticity based on these results is extremely small, approximately −0.02, indicating that the level of copayment rate has a negligible effect on the intensive margin of outpatient healthcare utilization |
| Lu Y, et al. (39) | 2023 | Prospective cohort study | 19 municipalities/people aged ≥65 years who were not certified as requiring long-term care | Social survey data (self-questionnaire) | Nonrecipients | 73,262 (Not available) | Functional disability over 5 years | In the ridge regression model, the characteristic of households receiving PA was an important predictor of functional disability |
| Miyake H, et al. (40) | 2023 | Cross-sectional study | Single center/patients with rheumatoid arthritis | Survey data, administered by healthcare providers to the patients or their representatives | Nonrecipients | 991 (17/974) | Polypharmacy and excessive polypharmacy | Excessive polypharmacy, defined as regularly taking 10 or more orally administered medications, was associated with the presence of PA (OR: 3.80, 95% CI: 1.23-11.72). |
| Miyake H, et al. (41) | 2023 | Cross-sectional study | Single center/patients with systemic lupus erythematosus (SLE) | Survey data, administered by healthcare providers to the patients or their representatives | Nonrecipients | 261 (8/253) | Polypharmacy and excessive polypharmacy | Excessive polypharmacy was associated with the presence of PA (multivariable OR: 18.9, 95% CI: 3.30-102.65) |
| Miyake H, et al. (42) | 2023 | Cross-sectional study | Single center/patients with rheumatoid arthritis | Survey data, administered by healthcare providers to the patients or their representatives | Nonrecipients | 991 (17/974) | Vaccination | Influenza vaccine: PA was significantly associated with nonvaccination |
| Nakamura Y, et al. (43) | 2023 | Case-control study | Single center/those who visited the Department of Psychiatry and Neurology | Medical records | Never received PA | 536 (87/449) | Medical visit behavior as a proxy for medication adherence | History of PA receipt was associated with higher nonattendance (OR: 2.04, 95% CI: 1.22-3.43, p = 0.007) |
| Kino S, et al. (44) | 2024 | Cross-sectional study | 60 municipalities/older community-dwelling recipients | Social survey data (self-questionnaire) | Nonrecipients | 16,366 (229/16,137) | Dental visits | In the fully adjusted model, PA recipients were 24% less likely to have dental visits for any reason (prevalence ratio [95% CI], 0.76 [0.64-0.90]), 23% less likely for treatment (0.77 [0.65-0.92]), and 21% less likely for prevention [0.79 (0.65-0.95]) |
| Kushibuchi M, et al. (67) | 2024 | Retrospective cohort study | Single center/patients diagnosed with alcoholic liver cirrhosis | Medical records | Nonrecipients | 244 (62/182) | All-cause mortality | The overall mortality rates were 48.4% and 31.9% for PA and non-PA recipients, respectively (p = 0.002). In the Cox regression model adjusted for age, ALBI score, HCV infection, and presence or absence of a designated key family contact, the hazard ratio for PA status was 1.75 (95% CI: 1.03-2.98, p = 0.039) |
A total of 13 studies used public assistance recipients as their study population (45), (46), (47), (48), (49), (50), (51), (52), (53), (54), (55), (56), (68). Among them, one study used data from the Japanese national database, which identified regional differences in the prevalence of admission length in psychiatric hospital (45) by public assistance recipients and its predictors. Furthermore, eight studies used data from public assistance databases of the welfare offices of local governments (46), (48), (49), (50), (51), (53), (55), (56). Among the public assistance recipients, several characteristics were associated with undesirable health statuses and behaviors. For example, those living alone or unemployed were more likely to have diabetes and frequently attend medical consultations (46), (49), (51), (53). Four studies used data obtained from a self-questionnaire social survey (47), (52), (54), (68). The health behavior scale of older recipients living alone, who have the most disadvantageous health risks among recipients, was developed (47) and examined for validity (54). This scale is reportedly useful in predicting the health behaviors of older recipients living alone, such as health checkup (47), (54). High activity of daily living and social capital were found to be associated with the initiation and termination of public assistance (Table 2) (52), (68).
Table 2. Descriptive Information on the Studies Using Public Assistance as an Entire Study Population.
| Authors | Year | Design | Settings/participants | Data | N | Outcome | Findings |
|---|---|---|---|---|---|---|---|
| Okumura Y, et al. (45) | 2019 | Cross-sectional study | All PA recipients hospitalized in psychiatric hospitals | National database | 46,559 | Age-sex-standardized claim ratio of the psychiatric admission | There is a geographical (prefectural) variation in the number and total medical cost of psychiatric admissions among recipients. There is a positive correlation between recipients’ psychiatric admission, the number of prefectural psychiatric beds per 100,000 population, and the prefectural proportion of the population receiving PA |
| Nishioka D, et al. (46) | 2020 | Retrospective cohort study | Adult recipients in two municipalities in Japan (>=20 years old) | Municipal database | 6,016 | Frequent outpatient attendance | Recipients living alone had an incidence of 1.58 (95% CI: 1.05-2.39) compared with those not living alone. Recipients visiting private institutions had an incidence of 1.74 (95% CI: 1.20-2.52) compared with those visiting medical corporations |
| Isozaki A, et al. (47) | 2021 | Cross-sectional study | Randomly sampled older recipients in Japan | Social survey data (self-questionnaire) | 1,280 | Health checkup behavior | The health behavior scale was developed, including two constructs (self-perception of personal power and practical skills for daily health), which correlates with recipients’ health checkup behavior |
| Nishioka D, et al.(48) | 2021 | Retrospective cohort study | Children in the household receiving PA in two municipalities in Japan (<=15 years old) | Municipal database | 573 | Children’s acute and chronic diseases | Among PA recipients, living in single parenthood is associated with a higher prevalence of the following: Asthma (IR: 1.62, 95% CI: 1.16-2.26) Allergic rhinitis (IR: 1.41, 95% CI: 1.07-1.86) Dermatitis and eczema (IR: 1.81, 95% CI: 1.21-2.7) Dental diseases (IR: 1.79, 95% CI: 1.33-2.42) An insignificant association was observed between single parenthood and children’s acute health conditions |
| Nishioka D, et al. (49) | 2021 | Retrospective cohort study | Adult recipients in two municipalities in Japan (>=20 years old) | Municipal database | 2,698 younger adults (20-64 years old) and 3,019 older adults (>65 years old) | 1-year cumulative incidence of diabetes diagnosis | Among younger (20-64 years old) men, the incidence of diabetes diagnosis was higher among those who were: Unemployed (IR: 1.28, 95% CI: 0.85-1.91) Living alone (IR: 1.48, 95% CI: 0.96-2.29). However, no significant association was observed among young women and older recipients |
| Nishioka D, et al. (50) | 2021 | Retrospective cohort study | Households receiving PA to rear children in five municipalities | Municipal database | 4,893 households | Households’ healthcare costs | Government savings through income reduction were counterbalanced by increased medical expenditure among child-rearing individuals in poverty (i.e., a 50 USD reduction in cash benefits may lead to a 248.6 USD increase in healthcare costs per household [95% CI: 25.4-471.7]) |
| Nishioka D, et al. (51) | 2021 | Retrospective cohort study | Adult recipients in two municipalities in Japan (>=20 years old) | Municipal database | 4,497 | Dental care access | Recipients who were younger (IR: 0.87 [by 10 years old], 95% CI: 0.84-0.91), women (IR: 1.22, 95% CI: 1.08-1.38), immigrants (IR: 1.53, 95% CI: 1.16-2.01), and with mental disabilities (IR: 1.30, 95% CI: 1.08-1.56) may have greater accessibility to dental care. Living alone and employment are potential predictors of dental care access. |
| Kino S, et al. (68) | 2022 | Retrospective cohort study | Older community-dwelling recipients | Social survey data (self-questionnaire) | 347 | Starting or leaving PA program | People with higher perceived mutual community help were 1.21 times (95% CI: 1.02-1.46) more likely to commence PA 3 years later than those who did not. PA recipients who felt community attachment to their resident community were 1.16 times more likely to give up PA 3 years later than those who did not (95% CI: 1.06-1.28). Similarly, those who had social roles were 1.15 times more likely to give up PA 3 years later than those who had not (95% CI: 1.01-1.30). |
| Kino S, et al. (52) | 2022 | Retrospective cohort study | Older community-dwelling recipients | Social survey data (self-questionnaire) | 335 | Changes in social relationships | Recipients who stopped receiving PA experienced an increase in the number of friends, frequency of meetings with friends, and participation in sports and hobby clubs. Conversely, the social relationships of nonrecipients in 2013 who started to receive PA in 2016 did not significantly change. |
| Nishioka D, et al. (53) | 2022 | Retrospective cohort study | Recipients in six municipalities in Japan | Municipal database | 15,739 | Frequent outpatient attendance (FOA) | Using CART analyses, the employed subpopulation with mental disabilities exhibited the highest risk of FOA (incidence proportion: 16.7%). Conventional regression analyses revealed that being unemployed was significantly associated with frequent outpatient attendance (IR: 1.71, 95% CI: 1.13-2.59). Living alone was also a predictor in regression analyses but not in CART analyses. |
| Imamatsu Y, et al. (54) | 2023 | Cross-sectional study | Randomly sampled older recipients in Japan | Social survey data (self-questionnaire) | 1,608 | Health behavior scale for older adults living alone and receiving PA (HBSO) | Recipients with higher Lubben social network scale scores have more preferable HBSO scores. A health checkup was also a predictor of a higher HBSO |
| Nishioka D, et al. (55) | 2023 | Retrospective cohort study | Adult recipients in two municipalities in Japan (>=20 years old) | Municipal database | 2,386 | Unscheduled asthma visits | Among working recipients, the IRs of unscheduled visits were higher among recipients cohabiting with adults (IR: 1.90, 95% CI: 1.00-3.59) and recipients cohabiting with children (IR: 2.35, 95% CI: 1.11-4.95) than among recipients living alone. Among the nonworking recipients, the IRs of unscheduled visits were lower among recipients living with family (IR: 0.74, 95% CI: 0.41-1.35) and those living with children (IR: 0.50, 95% CI: 0.20-1.23) than among recipients living alone |
| Ueno K, et al. (56) | 2023 | Cross-sectional study | Older recipients in two municipalities in Japan (>=65 years old) | Municipal database | 3,165 | Clustering older recipients using the soft clustering method | Employing a soft clustering technique can help identify meaningful segments among older recipients, which is useful in considering support measures for the recipients |
Eight studies used the proportion of the population receiving public assistance as a variable to express environmental factors across prefectures. Among these studies, only one used the proportion of the population receiving public assistance as a community-level economic factor in a cohort study (60). This study demonstrated that among men, the risk of cancer-related death was significantly higher with an increase in the proportion of households receiving public assistance. Seven were ecological studies (57), (58), (59), (61), (62), (63), (64). Considering the nature of ecological studies, it is inappropriate to apply the evidence to individual public assistance recipients, as people living in prefectures with a higher proportion of the population receiving public assistance tend to have unfavorable health conditions. Yoshikawa et al. reported that the COVID-19 incidence and mortality rates were higher in prefectures with a high proportion of the population receiving public assistance (Table 3) (63).
Table 3. Descriptive Information on the Studies Using the Proportion of the Population Receiving PA as an Environmental Predictor in Ecological Studies Included in the Scoping Review.
| Authors | Year | Design | Settings/data | N | Outcome | Findings |
|---|---|---|---|---|---|---|
| Aihara H, et al. (57) | 2002 | Ecological study | Yearly Annual Report of Hygiene in Osaka | 5 areas in Osaka City | The Standardized Mortality Ratio (SMR) of suicide (standardization to the 1980 Japanese population) in each area in Osaka | Among young (<40 years old) and middle-aged (40-64 years old) men, the number of persons per household and the availability of PA were associated with a higher SMR of suicide Among middle-aged (40-64 years old) women, the suicide rate was associated with the number of PA recipients per 1,000 persons for the period between 1980 and 1999 A real difference in association between the number of persons per household, the PA, and SMR in suicide was observed in Osaka prefecture |
| Aihara H, et al. (58) | 2003 | Ecological study | Yearly vital statistics for Japan | 47 prefectures | The SMR of suicide (standardization to the 1980 Japanese population) in each prefecture | Multivariate regression analyses revealed that the male SMR of suicide was negatively associated with the number of persons per household and PA |
| Mishina H, et al. (59) | 2012 | Ecological study | Data from home visits in the area covered by Fushimi Health Center to 2,933 mothers who had given birth between December 1, 2008 and October 31, 2010 | 5 localities in Fushimi-ward in Kyoto City | The detection rate of postpartum depressive symptoms in mothers | The proportion of households receiving PA in the localities had a positive correlation with the detection rate of postpartum depressive symptoms (r = 0.90, P = 0.04) |
| Honjo K, et al. (60) | 2014 | A retrospective cohort study | Data from the Japan Collaborative Cohort Study for Evaluation of Cancer Risk (JACC Study), followed up from 1990 to 2006 in 45 municipalities | 35 municipalities | All-cause death, cardiovascular death, cancer death, and death from injury, toxicosis, or external causes | Among men, the risk of death from cancer was significantly higher in the prefecture with a higher proportion of households receiving PA (coefficient 0.150 with SE 0.063 per unit increase) |
| Minagawa Y, et al. (61) | 2017 | Ecological study | Prefectural data from a Comprehensive Survey of Living Conditions (Kokumin Seikatsu Kiso Chosa) in 2010 | 47 prefectures | Prefecture-specific disability-free life expectancy (DFLE) at 65 years of age in 2010 | The percentage of older people receiving PA in prefecture was negatively associated with DFLE at 65 for women only (men: −0.01, not significant; women: −0.30, p < 0.001 per 1% point increase) |
| Okui T, et al. (62) | 2021 | Ecological study | Prefectural data was aggregated from individual data in the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB) data in the period of 2015-2018 | 47 prefectures | Standardized claim ratio (SCR) of the number of multidrug prescriptions (number of simultaneous prescriptions of seven or more internal medicines) by prefectures | The number of PA recipients per 1,000 persons was positively and significantly associated with the SCR (standardized partial regression coefficient = 0.244, p = 0.038) |
| Yoshikawa Y, et al. (63) | 2021 | Ecological study | The data on the cumulative number of cases with positive COVID-19 test results and deaths at the prefectural and national levels was provided by the Ministry of Health, Labour and Welfare of Japan | 47 prefectures | Rate ratios of COVID-19 incidence and mortality across prefectures | In prefectures with the most socioeconomic disadvantages, indicated by a greater proportion of the population receiving PA, there were higher incidence (RRs 2.45, 95% CI: 2.43-2.48) and mortality (RRs 2.02, 95% CI: 1.88-2.18) |
| Okui T, et al. (64) | 2022 | Ecological study | Prefectural data aggregated from individual data in the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB) data in the period of 2015-2018 | 47 prefectures | SCR of the amount of diazepam, equivalent dose prescriptions by prefectures | The number of PA recipients per capita was positively and significantly associated with the SCR (0.296, 95% CI: 0.0072-0.522) in hypnotics and (0.284, 95% CI: 0.096-0.476) in anxiolytics by a unit increase |
| PA, public assistance | ||||||
To the best of our knowledge, this was the first review to describe the health status of impoverished individuals receiving public assistance in Japan. The review included 56 studies, and we elucidated that the available evidence on the health status of public assistance recipients was based on observational data, including national and governmental data, social surveys, and hospital-based registration data. We found that public assistance recipients tended to have a more disadvantageous health and well-being statuses than the general population and that the prevalence of health outcomes varied across prefectures among the recipients. Focusing on people receiving public assistance, sociodemographic inequalities in health outcomes across recipients’ characteristics, such as household composition and employment status, were found. The proportion of the population receiving public assistance may be available as a prefectural monitoring measure or as an adjustment measure of community-level economic factors in public health studies in Japan.
As mentioned, descriptions of the health statuses of public and social assistance recipients have globally accumulated in recent years. Global evidence, excluding the Japanese population, has indicated that recipients have poorer health outcomes and problematic health behaviors than the general population not receiving public or social assistance (12), (69), (70). The present review identified that the health status of public assistance recipients in Japan was consistent with previous global evidence; thus, global evidence may also be applicable to these recipients. Shahidi et al. suggested that the use of public/social assistance programs may not be sufficiently protective for the health of impoverished individuals (12), (69). From the perspective of multidimensional poverty (11), additional social support beyond financial support for public assistance recipients in Japan may also be necessary to maintain the health of recipients.
The studies included in this review have several strengths and limitations. First, studies that utilized public assistance as an exposure variable focused on marginalized populations in which ordinary social surveys could not have been sufficiently outreached. However, these studies could only capture potential associations between the receipt of public assistance and health outcomes. Second, evidence based on studies using public assistance as a study population that used national and local governmental data had the strength of analyzing complete demographic data with few missing data; however, there were limitations in the generalizability of the findings due to the limited number of municipalities included in the review. Furthermore, the evidence included in this study indicates that public assistance recipients have more undesirable health risks than the general population, and a missing link regarding the mechanism that produces health inequality across the population remains unknown. When compared between public assistance recipients and nonrecipients, several studies have shown controversial results, with inverse or no association for health outcomes (14), (17), (18), (28), (32), (34). This may be due to the effect of the public assistance as social security on access to health care and the effect of social welfare support related to the public assistance system. However, each study is specific to its target population, and the results are extremely limited, requiring further studies with diverse population to address the underlying mechanisms. In addition, as public assistance recipients differ from the general population in their characteristics and the social context leading to their receipt of public assistance, studies that remove these biases and estimate causal relationships are needed.
More detailed socioeconomic status information on the daily lifestyles of public assistance recipients and longitudinal observations are needed to elucidate the mechanisms underlying the health problems of recipients. This may enable us to make more precise causal inferences regarding the modifying effects of public assistance on the relationship between poverty and health.
This review had several strengths and limitations. The results of this review were based on currently available robust evidence from peer-reviewed papers following a comprehensive literature search. However, we restricted our search to English-language publications. English-language publications have mainly been published in the last decade, and evidence may not have been sufficiently accumulated. Furthermore, the authors acknowledge the importance of reviewing Japanese-language publications; Japanese-language publications that quantitatively described the health and well-being statuses of the recipients were sparse (71), (72), (73), (74), (75). However, evidence from Japanese publications was consistent with the findings of this review and did not alter our conclusions.
In conclusion, public assistance recipients in Japan face more health risks than the general population, and the distribution of the risks is heterogeneous among recipients despite the minimum income protection and financial benefits in health and long-term care use. Further studies are warranted to identify the effect of public assistance policies on the impoverished population and to strategize effective support for recipients’ health. Evidence-based discussions and reforms of social security policies are imperative to protect individuals’ healthy lives, even when they fall into poverty.
This article is based on the study, which received the Medical Research Encouragement Prize of The Japan Medical Association in 2023.
None
This work was supported by [the Japan Society for the Promotion of Science KAKENHI] grant number [22K17404] and the [Health Labor Sciences Special Research Grant] grant number [23CA2001]. This work was supported by the Medical Research Encouragement Prize of The Japan Medical Association.
We thank Editage (www.editage.com) for the English language editing.
KH and DN conceptualized and designed the study. Both authors searched relevant literature and prepared the manuscript. All authors contributed equally to this study and approved the final version of the manuscript.
Not applicable.
Ottersen T, Norheim OF, World Health Organization Consultative Group on Equity and Universal Health Coverage. Making fair choices on the path to universal health coverage: Final report of the WHO Consultative Group on Equity and Universal Health Coverage. Bull World Health Organ. 2014;92(6):389.
World Health Organization. The Ottawa charter for health Promotion [Internet]. 1986 Nov [cited 2024 Mar 23]. Available from: http://www.who.int/healthpromotion/conferences/previous/ottawa/en/
International Conference on Primary Health Care. Declaration of Alma-Ata. WHO Chron. 1978;32(11):428-30.
Marmot M, Friel S, Bell R, et al. Closing the gap in a generation: health equity through action on the social determinants of health. Lancet. 2008;372(9650):1661-9.
Marmot M. Health equity in England: the Marmot review 10 years on. Bmj. 2020;368:m693.
Haushofer J, Fehr E. On the psychology of poverty. Science. 2014;344(6186):862-7.
Mani A, Mullainathan S, Shafir E, et al. Poverty impedes cognitive function. Science. 2013;341(6149):976-80.
OECD. Income inequality (indicator). OECD [Internet]. 2023 [cited 2024 Mar 23]. Available from: https://data.oecd.org/inequality/income-inequality.htm
The Constitution of Japan. Article 25. 1946 Nov [Internet]. [cited 2024 Mar 23]. Available from: https://www.refworld.org/legal/legislation/natlegbod/1946/en/13876
Sakamoto H, Rahman M, Nomura S, et al. Japan health system review. Health Syst Transit. 2018;8(1):228.
Spicker P. Definitions of poverty: twelve clusters of meaning. Poverty: an international glossary; 2007. p. 229-43.
Shahidi FV, Ramraj C, Sod-Erdene O, et al. The impact of social assistance programs on population health: a systematic review of research in high-income countries. BMC Public Health. 2019;19(1):2.
Noda T, Imamichi H, Kawata A, et al. Long-term outcome in 306 males with alcoholism. Psychiatry Clin Neurosci. 2001;55(6):579-86.
Kobayashi O, Matsumoto T, Otsuki M, et al. Profiles associated with treatment retention in Japanese patients with methamphetamine use disorder: preliminary survey. Psychiatry Clin Neurosci. 2008;62(5):526-32.
Wada T, Moriya T, Iba K, et al. Functional outcomes after arthroscopic treatment of lateral epicondylitis. J Orthop Sci. 2009;14(2):167-74.
Kamimura A, Yoshihama M, Bybee D. Trajectory of intimate partner violence and healthcare seeking over the life course: study of Japanese women in the Tokyo metropolitan area, Japan. Public Health. 2013;127(10):902-7.
Uchimura K, Ngamvithayapong-Yanai J, Kawatsu L, et al. Permanent employment or public assistance may increase tuberculosis survival among working-age patients in Japan. Int J Tuberc Lung Dis. 2015;19(3):312-8.
Takenaka Y, Yasui T, Enomoto K, et al. Health insurance status and survival among patients with head and neck cancer in Japan. Int J Clin Oncol. 2016;21(3):517-22.
Funakoshi M, Azami Y, Matsumoto H, et al. Socioeconomic status and type 2 diabetes complications among young adult patients in Japan. PLOS ONE. 2017;12(4):e0176087.
Kawahara YY, Hashimoto S, Harada M, et al. Predictors of short-term repetition of self-harm among patients admitted to an emergency room following self-harm: a retrospective one-year cohort study. Psychiatry Res. 2017;258:421-6.
Nakanishi M, Endo K, Ando S. The basic act for suicide prevention: effects on longitudinal trend in deliberate self-harm with reference to national suicide data for 1996-2014. Int J Environ Res Public Health. 2017;14(1):104.
Yuda M. The medical assistance system and inpatient health care provision: empirical evidence from short-term hospitalizations in Japan. PLOS ONE. 2018;13(10):e0204798.
Izumi K, Murase Y, Uchimura K, et al. Transmission of tuberculosis and predictors of large clusters within three years in an urban setting in Tokyo, Japan: a population-based molecular epidemiological study. BMJ Open. 2019;9(5):e029295.
Cho T, Aoki S, Saigusa Y, et al. Risk factors for chlamydia trachomatis infection and preterm birth in pregnant Japanese women: does chlamydial infection cause preterm birth? Jpn J Infect Dis. 2020;73(3):210-3.
Kaneko M, Inoue M, Okubo M, et al. Differences between frequent emergency department users in a secondary rural hospital and a tertiary suburban hospital in central Japan: a prevalence study. BMJ Open. 2020;10(9):e039030.
Osawa I, Sato T, Goto T, et al. Characteristics and subgroups of frequent emergency department users in an academic hospital in Japan. Acute Med Surg. 2020;7(1):e535.
Yoshikawa R, Kawatsu L, Uchimura K, et al. Delay in health-care-seeking treatment among tuberculosis patients in Japan: what are the implications for control in the era of universal health coverage? Western Pac Surveill Response J. 2020;11(2):37-47.
Kaneko M, Watanabe T, Fujinuma Y, et al. Overall mortality in older people receiving physician-led home visits: a multicentre prospective study in Japan. Fam Pract. 2021;38(4):395-402.
Koyama Y, Fujiwara T, Isumi A, et al. The impact of public assistance on child mental health in Japan: results from A-CHILD study. J Public Health Policy. 2021;42(1):98-112.
Watanabe S, Usui M. Clinical features of ST-segment elevation myocardial infarction in patients receiving welfare public assistance in urban area of Japan. J Cardiol. 2021;77(4):404-7.
Fujito H, Kitano D, Saito Y, et al. Association between the health insurance status and clinical outcomes among patients with acute heart failure in Japan. Heart Vessels. 2022;37(1):83-90.
Kaneko M, Shinoda S, Shimizu S, et al. Fragmentation of ambulatory care among older adults: an exhaustive database study in an ageing city in Japan. BMJ Open. 2022;12(8):e061921.
Kino S, Nishioka D, Ueno K, et al. Public assistance program and depressive symptoms of the recipient: a cross-sectional Japan gerontological evaluation study. BMC Geriatr. 2022;22(1):177.
Nishimoto Y, Kato T, Morimoto T, et al. Public assistance in patients with acute heart failure: a report from the KCHF registry. ESC Heart Fail. 2022;9(3):1920-30.
Nakayama T, Nishioka K, Uchiyama K, et al. Late Dialysis modality education could negatively predict peritoneal dialysis selection. J Clin Med. 2022;11(14):4042.
Sengoku T, Ishizaki T, Goto Y, et al. Prevalence of type 2 diabetes by age, sex and geographical area among two million public assistance recipients in Japan: a cross-sectional study using a nationally representative claims database. J Epidemiol Community Health. 2022;76(4):391-7.
Wakata S, Nishioka D, Takaki Y. Changes in health-related quality of life scores among low-income patients on social welfare programs in Japan during the COVID-19 pandemic: a single-center repeated cross-sectional study. BMC Public Health. 2022;22(1):2147.
Yuda M. Healthcare utilization under a comprehensive public welfare program: evidence from Japan. Front Public Health. 2022;10:895679.
Lu Y, Sato K, Nagai M, et al. Machine learning-based prediction of functional disability: a cohort study of Japanese older adults in 2013-2019. J Gen Intern Med. 2023;38(11):2486-93.
Miyake H, Sada RM, Akebo H, et al. Prevalence and factors associated with polypharmacy among patients with rheumatoid arthritis: a single-centre, cross-sectional study. Clin Rheumatol. 2023;42(9):2287-95.
Miyake H, Sada RM, Akebo H, et al. Polypharmacy prevalence and associated factors in patients with systemic lupus erythematosus: a single-centre, cross-sectional study. Mod Rheumatol. 2023;34(1):106-12.
Miyake H, Sada RM, Tsugihashi Y, et al. Single-centre, cross-sectional study on the factors and reasons for non-vaccination among patients with rheumatoid arthritis. Mod Rheumatol. 2023;34(1):79-86.
Nakamura Y, Sakurai K, Ishikawa S, et al. Outpatient visit behavior in patients with epilepsy: generalized epilepsy is more frequently non-attendance than focal epilepsy. Epilepsy Behav. 2023;145:109345.
Kino S, Ueno K, Nishioka D, et al. Prevalence of dental visits in older Japanese adults receiving public assistance. Community Dent Oral Epidemiol. 2024;52(1):68-75.
Okumura Y, Sakata N, Tachimori H, et al. Geographical variation in psychiatric admissions among recipients of public assistance. J Epidemiol. 2019;29(7):264-71.
Nishioka D, Saito J, Ueno K, et al. Frequent outpatient attendance among people on the governmental welfare programme in Japan: assessing both patient and supplier characteristics. BMJ Open. 2020;10(10):e038663.
Isozaki A, Tadaka E. Development of a health behavior scale for older adults living alone receiving public assistance. BMC Public Health. 2021;21(1):1428.
Nishioka D, Saito J, Ueno K, et al. Single-parenthood and health conditions among children receiving public assistance in Japan: a cohort study. BMC Pediatr. 2021;21(1):214.
Nishioka D, Saito J, Ueno K, et al. Non-financial social determinants of diabetes among public assistance recipients in Japan: a cohort study. J Diabetes Investig. 2021;12(6):1104-11.
Nishioka D, Takaku R, Kondo N. Medical expenditure after marginal cut of cash benefit among public assistance recipients in Japan: natural experimental evidence. J Epidemiol Community Health. 2021;76(5):505-11.
Nishioka D, Ueno K, Kino S, et al. Sociodemographic inequities in dental care utilisation among governmental welfare recipients in Japan: a retrospective cohort study. Int J Equity Health. 2021;20(1):141.
Kino S, Nishioka D, Ueno K, et al. Changes in social relationships by the initiation and termination of public assistance in the older Japanese population: a JAGES panel study. Soc Sci Med. 2022;293:114661.
Nishioka D, Kino S, Ueno K, et al. Risk profiles of frequent outpatients among public assistance recipients in Japan: a retrospective cohort study using a classification and regression trees algorithm. BMJ Open. 2022;12(5):e054035.
Imamatsu Y, Tadaka E. Factors associated with health behaviors in preventing non-communicable diseases among older adults living alone in poverty in Japan. Front Public Health. 2023;11:1207334.
Nishioka D, Saito J, Ueno K, et al. Sociodemographic inequities in unscheduled asthma care visits among public assistance recipients in Japan: additional risk by household composition among workers. BMC Health Serv Res. 2023;23(1):1084.
Ueno K, Nishioka D, Saito J, et al. Identifying meaningful subpopulation segments among older public assistance recipients: a mixed methods study to develop tailor-made health and welfare interventions. Int J Equity Health. 2023;22(1):146.
Aihara H, Iki M. Effects of socioeconomic factors on suicide from 1980 through 1999 in Osaka Prefecture, Japan. J Epidemiol. 2002;12(6):439-49.
Aihara H, Iki M. An ecological study of the relations between the recent high suicide rates and economic and demographic factors in Japan. J Epidemiol. 2003;13(1):56-61.
Mishina H, Yamamoto Y, Ito M. Regional variations in prevalence of postpartum depressive symptoms: population-based survey. Pediatr Int. 2012;54(4):563-5.
Honjo K, Iso H, Fukuda Y, et al. Influence of municipal- and individual-level socioeconomic conditions on mortality in Japan. Int J Behav Med. 2014;21(5):737-49.
Minagawa Y, Saito Y. An analysis of factors related to disability-free life expectancy at 65 years of age across Japanese prefectures in 2010. Eur J Ageing. 2018;15(1):15-22.
Okui T, Park J. Analysis of the regional difference in the number of multi-drug prescriptions and its predictors in Japan, 2015-2018. BMC Res Notes. 2021;14(1):367.
Yoshikawa Y, Kawachi I. Association of socioeconomic characteristics with disparities in COVID-19 outcomes in Japan. JAMA Netw Open. 2021;4(7):e2117060.
Okui T, Park J. Analysis of regional differences in the amount of hypnotic and anxiolytic prescriptions in Japan using nationwide claims data. BMC Psychiatry. 2022;22(1):44.
Ikeda K, Harada T, Tarumi Y, et al. Association between public assistance and frequent emergency department visits in urban areas of Japan: a case-control study. Showa Univ J Med Sci. 2020;32(1):73-80.
Kino S, Stickley A, Nishioka D, et al. Suicidal ideation and suicide attempts among older recipients of public welfare assistance in Japan. J Epidemiol Community Health. 2022;76(10):873-9.
Kushibuchi M, Okuse C, Ie K, et al. Limits of subsidized medical care in reducing the effect of socioeconomic disparities: liver cirrhosis mortality in Japan. J St Marianna Univ. 2023;14(1):1-12.
Kino S, Nishioka D, Ueno K, et al. Role of psychosocial factors in starting and leaving public assistance programs by older Japanese population: longitudinal Japan gerontological evaluation study. Arch Gerontol Geriatr. 2022;99:104615.
Shahidi FV, Muntaner C, Shankardass K, et al. The effect of welfare reform on the health of the unemployed: evidence from a natural experiment in Germany. J Epidemiol Community Health. 2020;74(3):211-8.
Sod-Erdene O, Vahid Shahidi F, Ramraj C, et al. Is social assistance boosting the health of the poor? Results from Ontario and three countries. Can J Public Health. 2019;110(4):386-94.
Saito J, Kondo N, Takagi D. [Factors related to health examination receipt among public assistance recipients: targeting basic attribute survey]. J Health Welf Stat. 2017;65(5):15-20. Japanese.
Matsunami Y, Kawai A. [Smoking among recipients of public assistance benefits from N city, and their recognition of smoking cessation therapy]. Jpn J Tob Control. 2015;10(4):51-8. Japanese.
Saito M, Fujita K, Hirano T, et al. [Stability and Change in the cost of care services due to premiums for longterm care insurance: from the data of individually provided care benefits in a specific municipality during two year]. J Soc Secur Res. 2011;47:293-303. Japanese.
Tomita S, Mitoku K, Nakajima T. [Associations between smoking and health-related behaviors of middle-aged public assistance recipients]. Jpn J Tob Control. 2016;11(4):114-20. Japanese.
Yamada S, Saito M, Yokoyama Y. [Differences in happiness among the elderly according to the status of public assistance receipt: cross-sectional data from JAGES 2013 and 2016]. Jpn J Soc Welf. 2023;63(4):15-26. Japanese.