Figure 1. Images
Computed tomography (CT) images
A) Head CT image revealed a low-intensity area at the left temporal lobe.
B) Cervical CT imaging showed lymphadenopathy from the left neck to the left axilla (arrow heads) and a continuous mass lesion in the left parotid glands (arrow).
C) Chest CT imaging showed bilateral pleural effusion and passive atelectasis, and infiltrative shadows in the bilateral upper lobe, middle lobe, and lingular segment.
Magnetic resonance (MR) images
D-a) Fluid-attenuated inversion recovery imaging of the brain revealed a high intensity in the left hippocampus, insula, and cingula, and edematous change of the left temporal lobe. Hyperintensity in the subarachnoid space of the right frontal lobe suggesting meningeal carcinomatosis (circle).
D-b) Diffusion-weighted imaging signal hyperintensity in the left pulvinar of the thalamus and hippocampus. These findings suggested NCSE.
From: Nonconvulsive Status Epilepticus Caused by Cerebrospinal Fluid Dissemination of a Salivary Duct Carcinoma: A Case Report
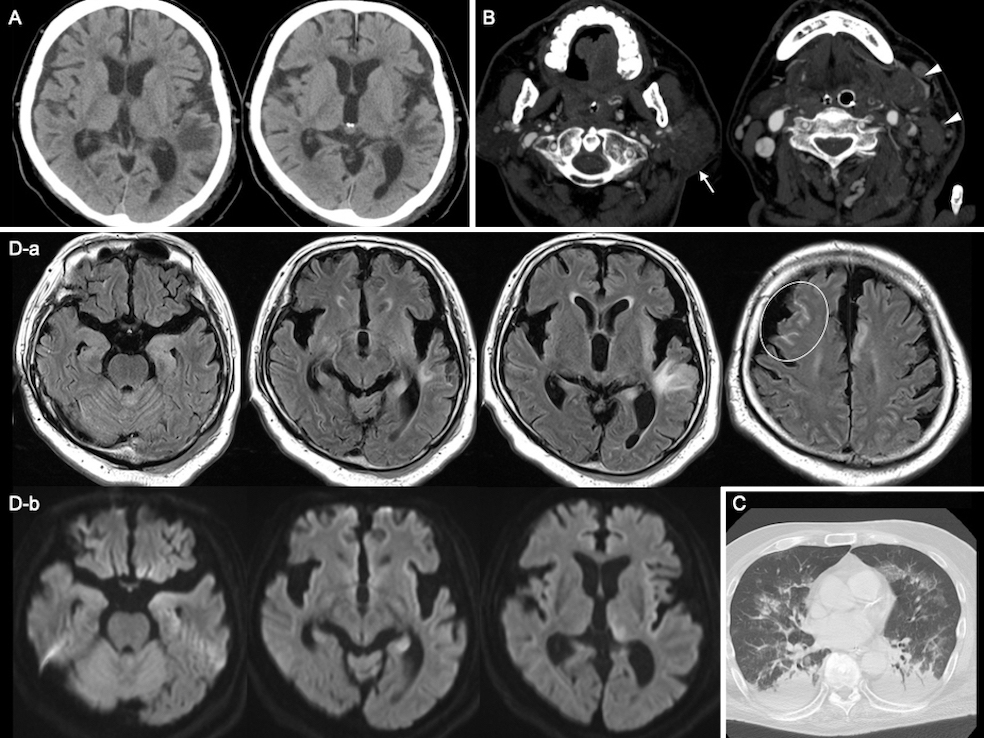
Figure 3. Electroencephalogram at the onset (A: the monopolar montage; B: the longitudinal bipolar montage) and after starting levetiracetam (C)
A, B) Lateralized rhythmic delta activity (LRDA) in the left frontal parietal region began as low-voltage 3 Hz blunt waves and changed to triphasic morphology. After that, lateralized periodic discharges (LPDs) with triphasic morphology appeared. The frequency fluctuated between 1.5 and 2 per second.
C) LRDA and LPDs disappeared, and alpha and theta waves at 7-9 Hz were irregular and unsteady.
From: Nonconvulsive Status Epilepticus Caused by Cerebrospinal Fluid Dissemination of a Salivary Duct Carcinoma: A Case Report
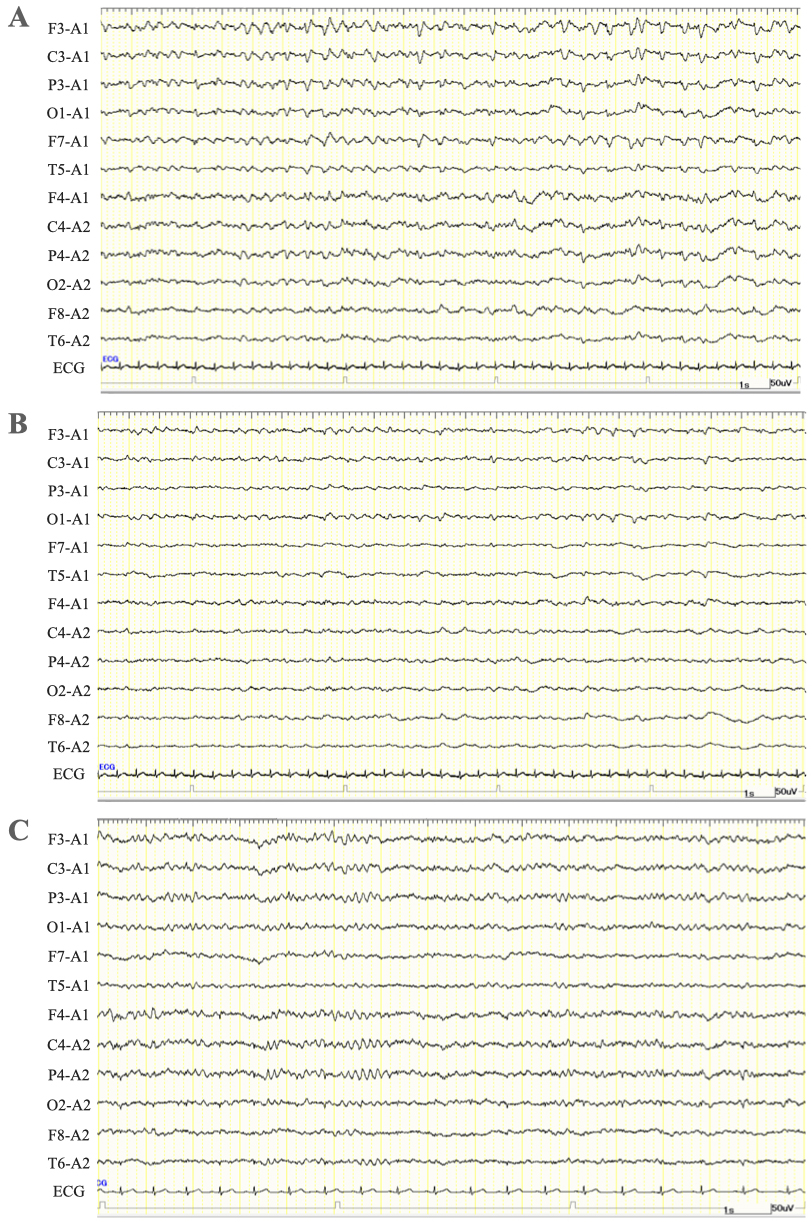
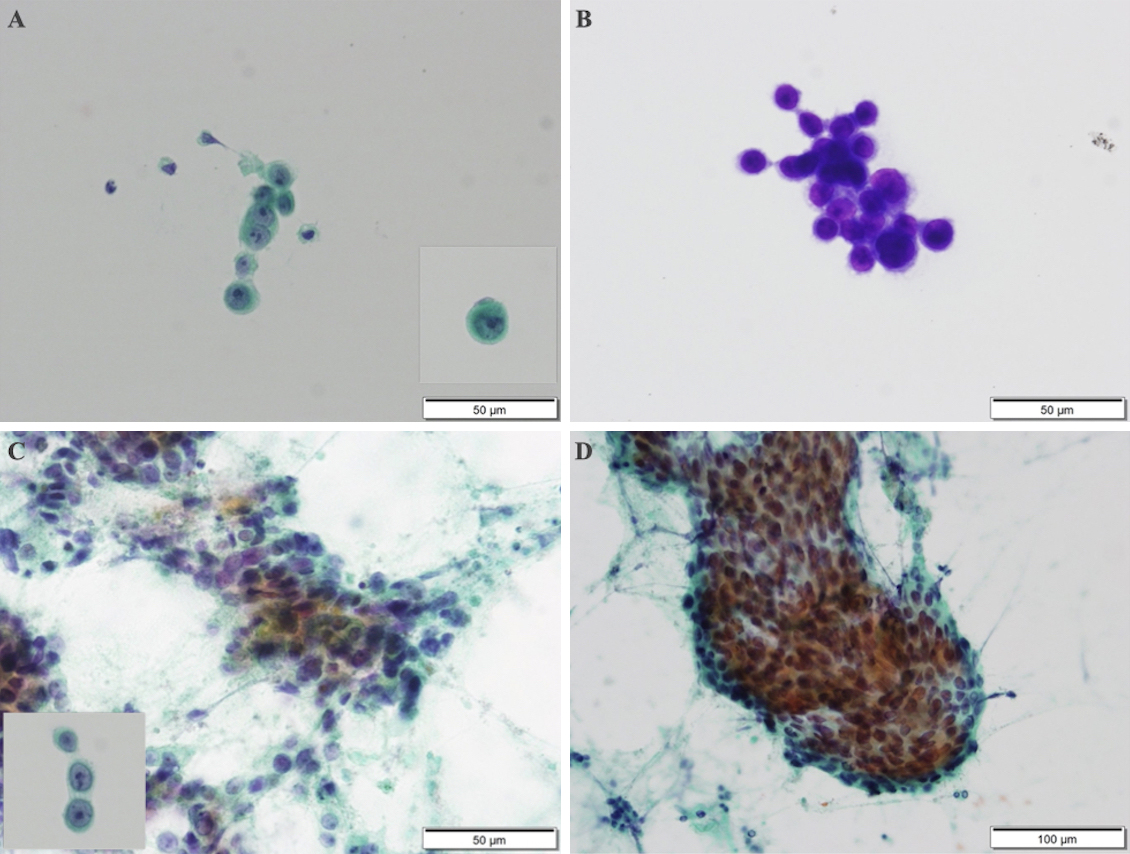
Figure 4. Cytodiagnosis of the cerebrospinal fluid
(A) Papanicolaou stain. Solitary or clustered large lymphoid cells with conspicuous nucleoli were determined.
(B) Periodic acid Schiff staining was positive, and adenocarcinoma was suspected.
Papanicolaou stain of the neck mass
(C) Colonization of the epidermal atypical cells was determined with a background of massive necrosis. Histopathological findings of the neck mass were similar to those of the cerebrospinal fluid.
(D) Tubular formations were determined.
From: Nonconvulsive Status Epilepticus Caused by Cerebrospinal Fluid Dissemination of a Salivary Duct Carcinoma: A Case Report