Figure 2. A. Hematoxylin-eosin staining of the gallbladder wall. Collagen fibers are stained pink and display growth. Significant infiltration of the lymphoplasmacytic cells. B. Immunoglobulin G4 (IgG4)-positive immunohistochemical image of the gallbladder wall. Infiltration of IgG4-positive plasma cells (stained brown) is observed. More than 40% of IgG-positive plasma cells were IgG4-positive, and these cells are >10 cells/high-power field.
From: Usefulness of Serum IgG4 and Thyroid Stimulating Hormone Levels in Differentiating Headache
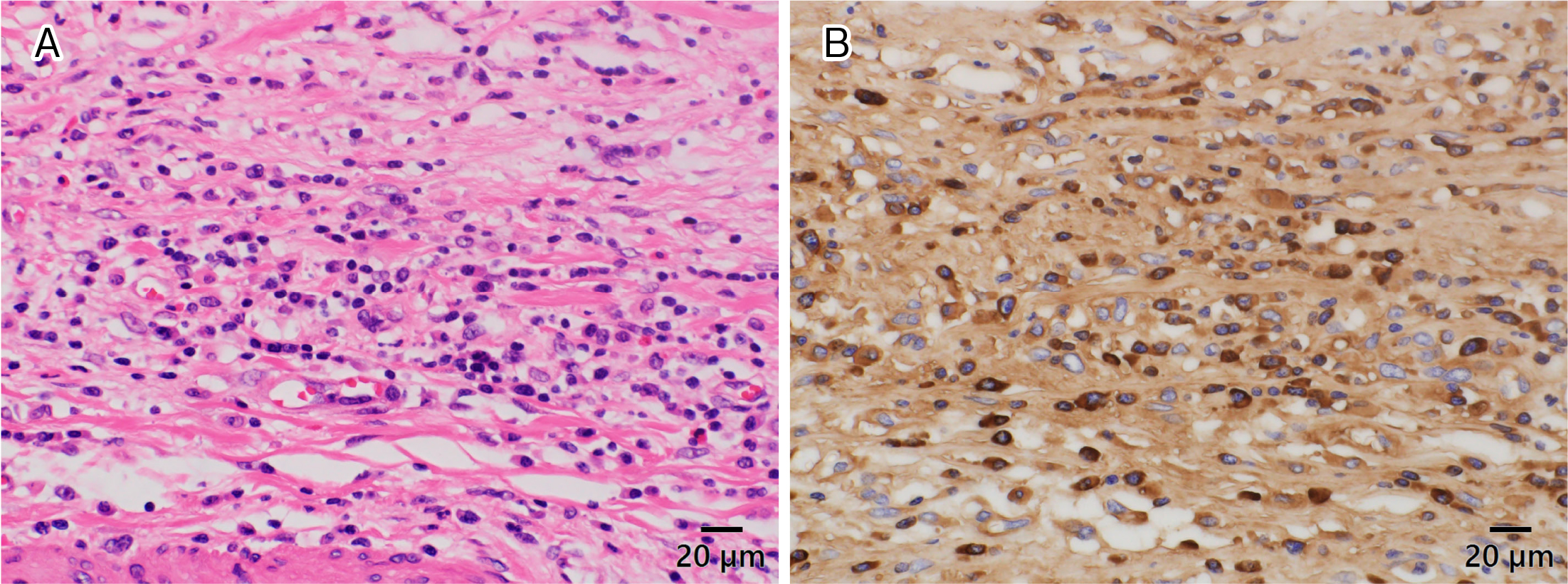
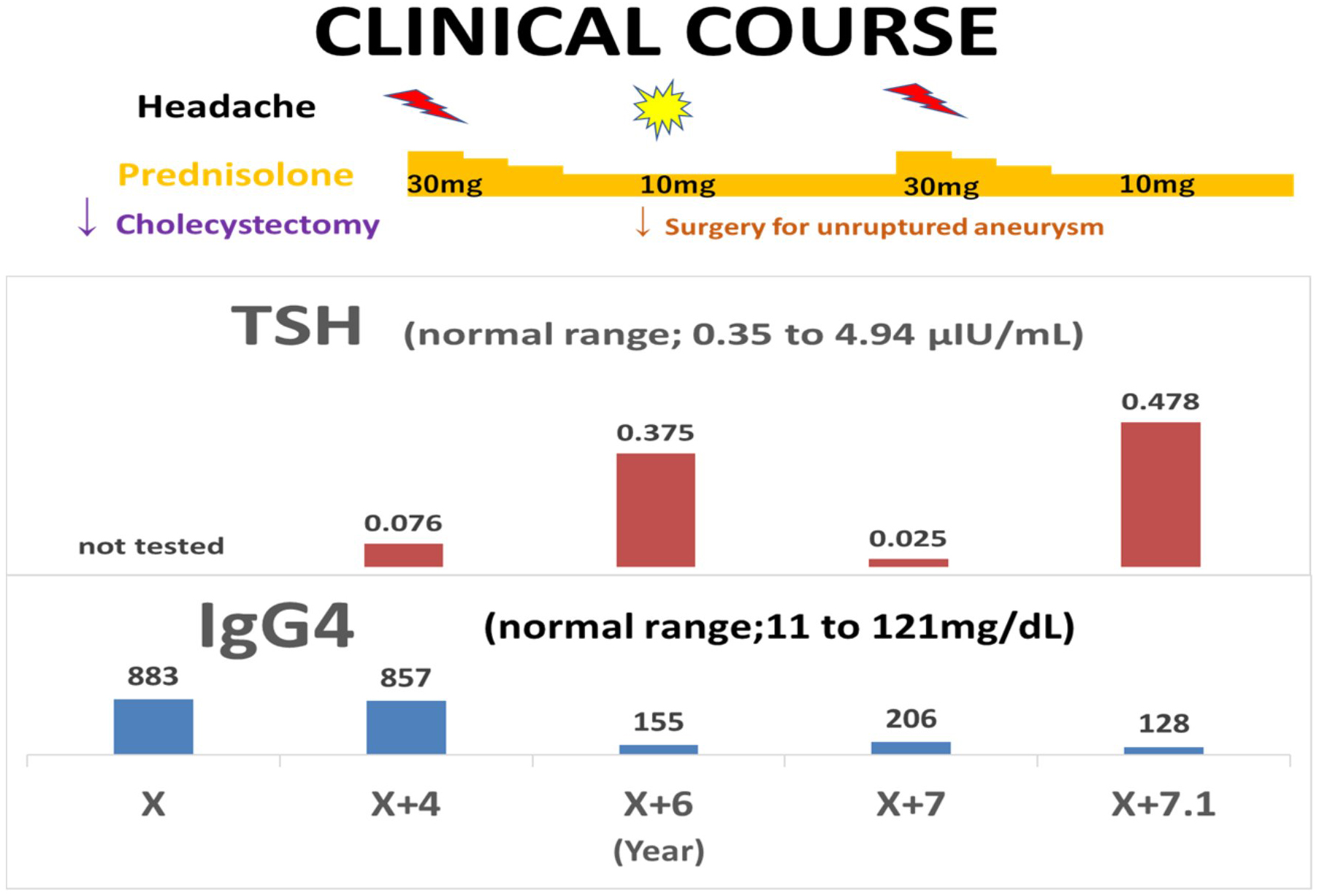
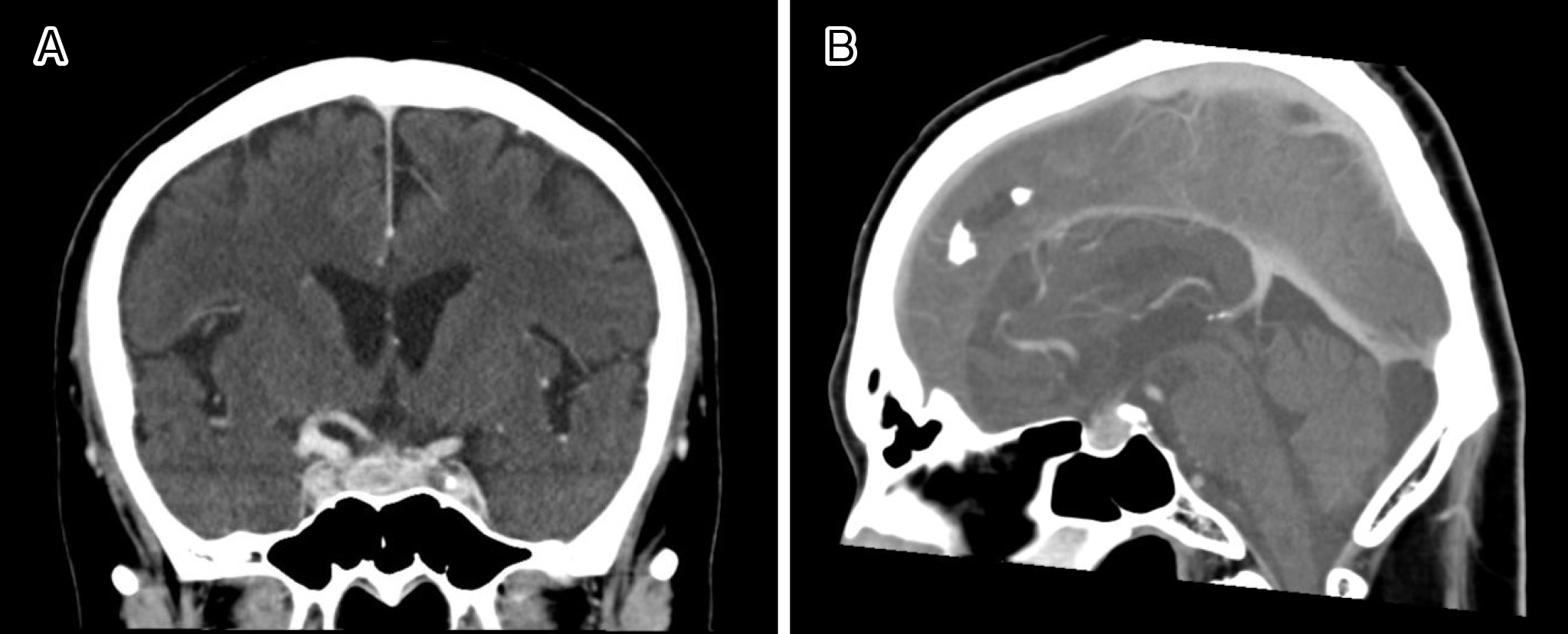
Figure 4. Clinical course of the patient. 25 μg/day of levothyroxin administration has been started since X + 4 years. The serum adrenocorticotropic hormone (ACTH) level was less than 2.0 pg/mL (N: 7.2-63.3) and the serum growth hormone (GH) level was 0.34 ng/mL (N: ≥2.47). In addition, the free T4 (FT4) level was 0.69 ng/dL (N: 0.7-1.7). A comparison of head computed tomography scans at X + 4 and X + 6 years suggested that prednisolone reduced the approximate pituitary volume by approximately one-half (1563 vs. 839 mm3).
From: Usefulness of Serum IgG4 and Thyroid Stimulating Hormone Levels in Differentiating Headache