Corresponding author: Yoshiyuki Nakatsuji, nakatsuji_y@marunouchi.or.jp
DOI: 10.31662/jmaj.2021-0220
Received: December 13, 2021
Accepted: March 3, 2022
Advance Publication: June 17, 2022
Published: July 15, 2022
Cite this article as:
Nakatsuji Y, Fukuzawa S, Arima I, Yamamoto K. Usefulness of Serum IgG4 and Thyroid Stimulating Hormone Levels in Differentiating Headache. JMA J. 2022;5(3):372-374.
Key words: IgG4-related disease, Hypophysitis, Cholecystitis, Thyroid stimulating hormone, Headache, Prednisolone
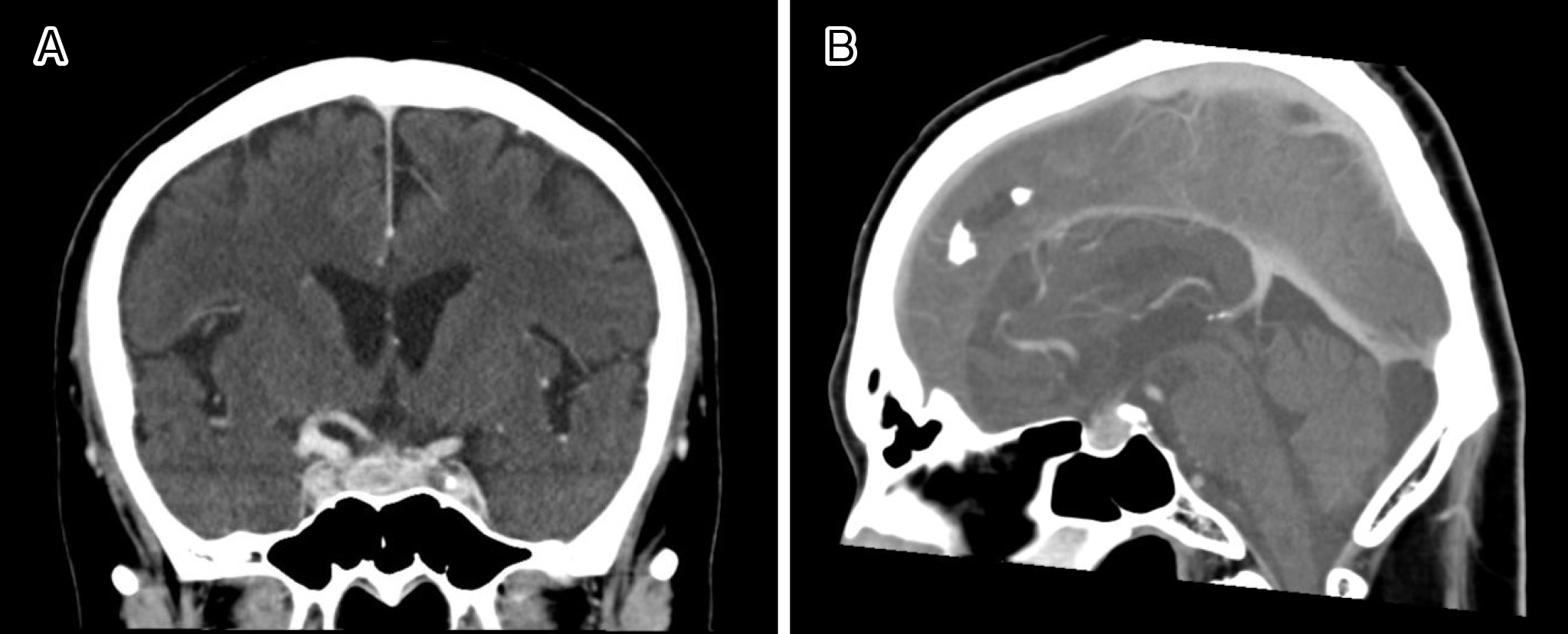
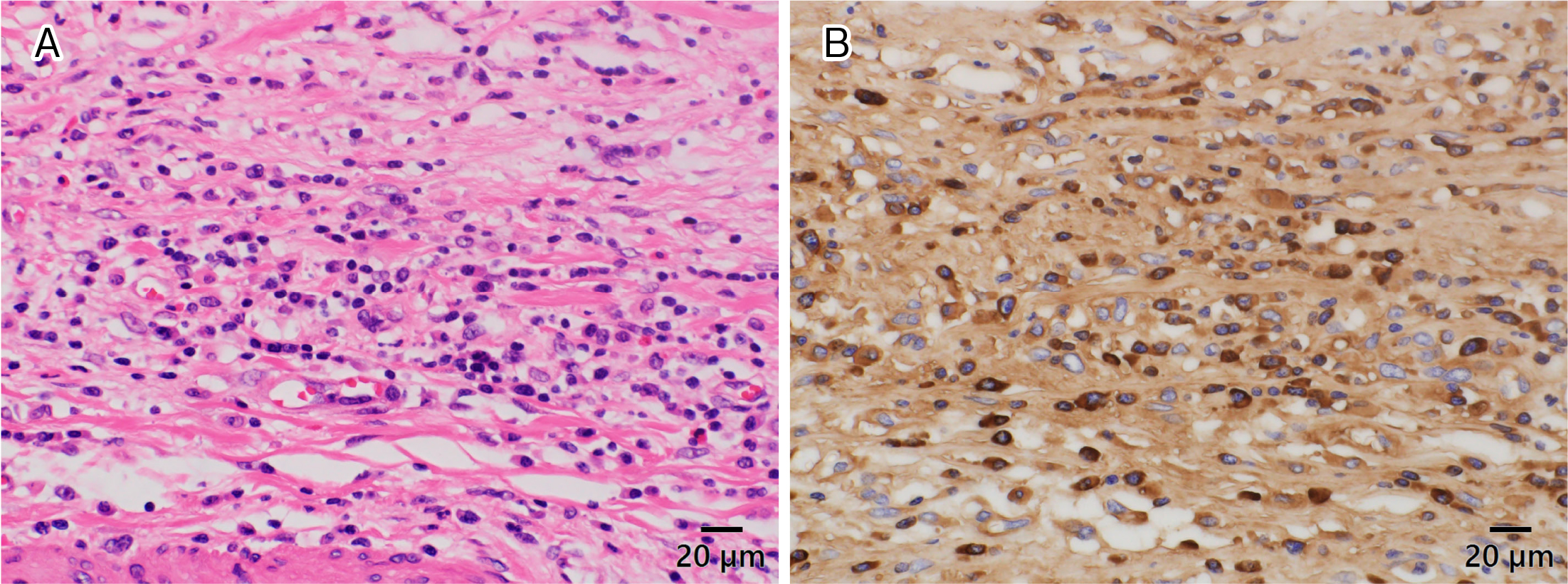
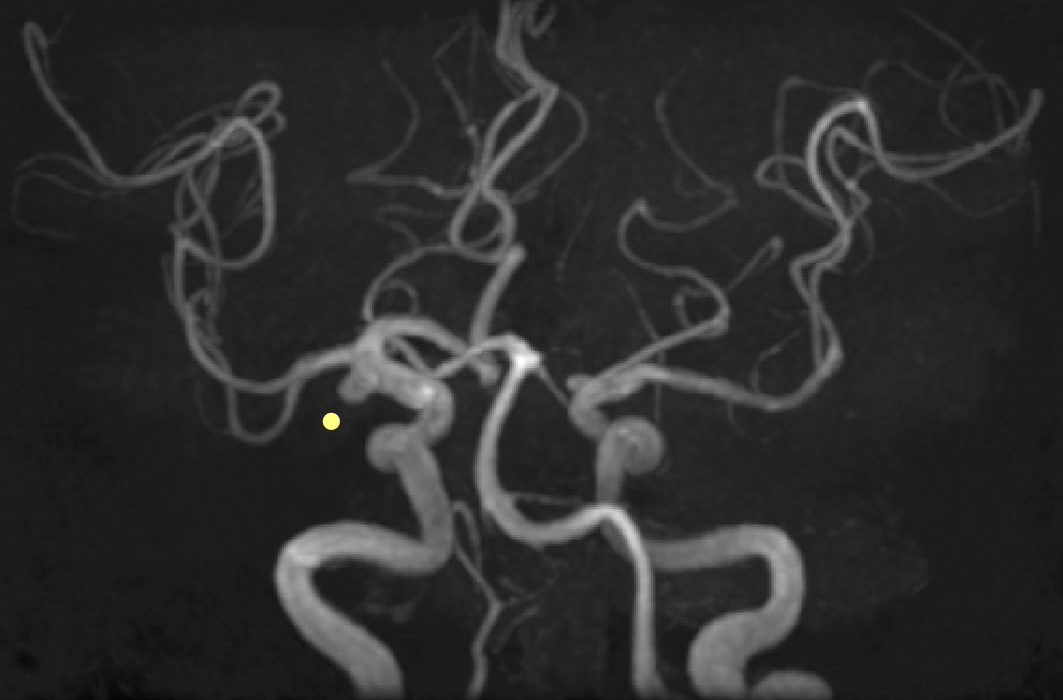
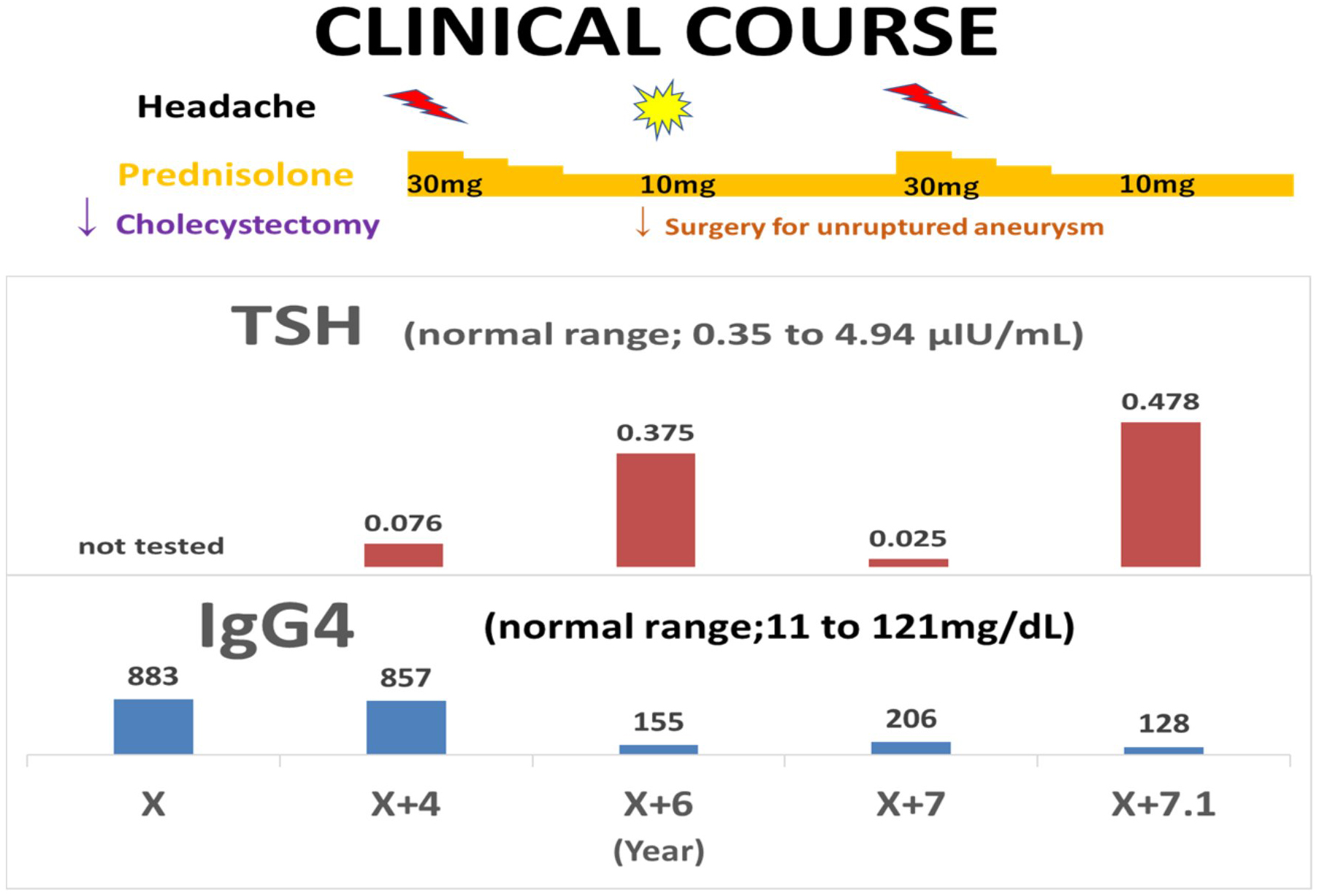
A 67-year-old man was admitted with a headache. He had a history of cholecystectomy for immunoglobulin G4 (IgG4)-related cholecystitis and hypophysitis, diagnosed 7 and 3 years ago, respectively. Moreover, a year ago, he underwent surgery for unruptured cerebral aneurysm. Hypophysitis diagnosis was based on pituitary enlargement observed on head contrast-enhanced computed tomography (Figure 1A and B), IgG4-positive cells in the gallbladder wall at cholecystectomy (Figure 2A and B), and high serum IgG4 levels (883 mg/dL) (1), (2). It was accompanied by headache and hypopituitarism, a substantial decrease in the thyroid stimulating hormone (TSH) level, which improved to normal levels following the administration of 30 mg/day prednisolone (3). Headache was present during cerebral aneurysm surgery (Figure 3: yellow dot); however, IgG4 and TSH levels remained stable. The aforementioned levels in X + 7 years were 206 mg/dL and 0.025 μIU/mL, respectively, which helped differentiating his headache and increasing the dosage of prednisolone (Figure 4) (4).
None
We thank Maki Miyata M.D. and Masahiro Agata M.D. at Ichinose Neurosurgical Hospital in Matsumoto for the neurosurgical operation of cerebral aneurysm. We also thank Jyun Igarashi M.D. at Department of Surgery of Marunouchi Hospital for performing cholecystectomy, Tsuyoshi Tada M.D. at Department of Neurosurgery of Marunouchi Hospital for his helpful discussion, and Masayoshi Hayama Ph.D. at Department of Clinical Pathology of Marunouchi Hospital for his fantastic work of histopathology. There are no sources of financial support.
Our manuscript has been edited by a native English speaker of editageⓇ.
YN planned and prepared this manuscript; SF and IA provided their support for preparing the article; KY provided support for submitting the tissue samples and helped finalizing the article.
This study did not require IRB approval.
Informed consent was obtained from patient to publish this case, including pictures.
Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344(10):732-8.
Umehara H, Okazaki K, Masaki Y, et al. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012;22(1):1-14.
Iseda I, Hida K, Tone A, et al. Prednisolone markedly reduced serum IgG4 levels along with the improvement of pituitary mass and anterior pituitary function in a patient with IgG4-related infundibulo-hypophysitis. Endocr J. 2014;61(2):195-203.
Bando H, Iguchi G, Fukuoka H, et al. The prevalence of IgG4-related hypophysitis in 170 consecutive patients with hypopituitarism and/or central diabetes insipidus and review of the literature. Eur J Endocrinol. 2014;170(2):161-72.
