Corresponding author: Kotaro Sugimoto, sugikota@fmu.ac.jp
DOI: 10.31662/jmaj.2020-0082
Received: October 2, 2020
Accepted: January 12, 2021
Advance Publication: March 2, 2021
Published: April 15, 2021
Cite this article as:
Yamashita R, Tanaka M, Chiba H, Sugimoto K. Bacterial Myocarditis in a Patient with Cancer. JMA J. 2021;4(2):169-170.
Key words: bacterial myocarditis, cardiac infection, histopathology
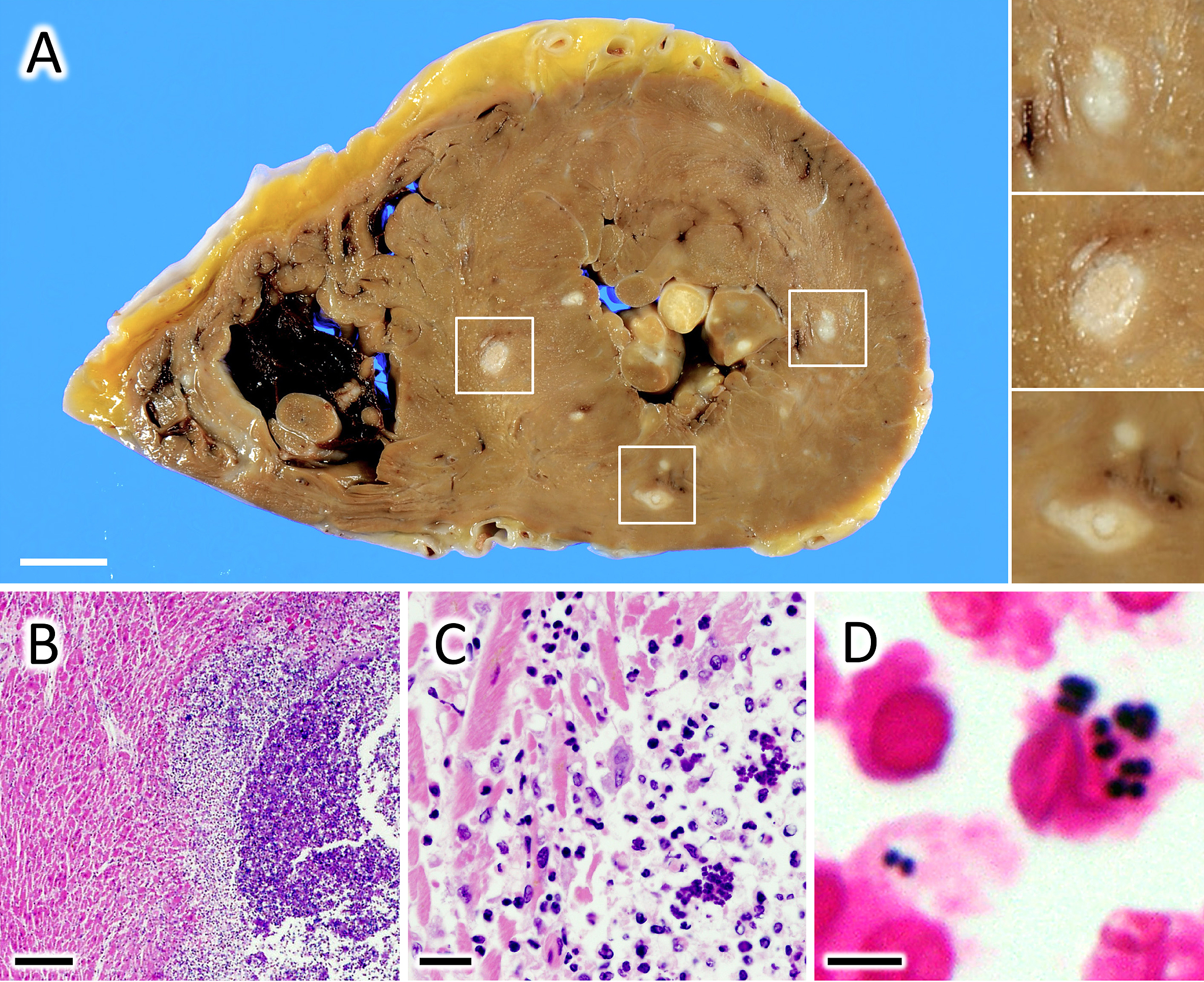
A 69-year-old man with stage IV esophageal cancer developed a sudden onset of fever and died of cardiopulmonary arrest. The patient had cachexia but was not in the terminal phase. Significant arrhythmia or malfunction of the heart had not been observed. An autopsy indicated that the tumor did not metastasize to any critical organs but only to the adrenal glands and peripheral lymph nodes. Meanwhile, hundreds of abscesses containing numerous gram-positive diplococci (Figure 1A, B, C and D ) were observed in the heart and lung. Thus, it was concluded that the patient died of bacterial myocarditis. Although spontaneous bacterial myocarditis is considered uncommon in developed countries, many pathogens causing pneumonia often trigger bacterial myocarditis. An autopsy study demonstrated that 40% of patients with lobar pneumonia had concomitant bacterial myocarditis (1), (2). Therefore, an understanding of the association between pneumonia and myocarditis would inform clinical practice, especially in the care for compromised patients.
None
RY, MT, HC, and KS performed the autopsy, prepared the specimens, and diagnosed the patient. RY and KS wrote the manuscript.
Informed consent was obtained from the patient’s family to publish this case, including pictures.
This study did not require IRB approval.
Corrales-Medina VF, Musher DM, Shachkina S, et al. Acute pneumonia and the cardiovascular system. Lancet. 2013;381(9865):496-505.
Saphir O, Amromin GD. Myocarditis in instances of pneumonia. Ann Intern Med. 1948;28(5):963-70.
