Corresponding author: Hirohisa Fujikawa, hirohisa.fujikawa@gmail.com
DOI: 10.31662/jmaj.2020-0121
Received: December 23, 2020
Accepted: February 12, 2021
Advance Publication: April 2, 2021
Published: April 15, 2021
Cite this article as:
Fujikawa H, Kokita A, Watanabe K, Saito M. Primary Splenic Lymphoma: An Uncommon Cause of Persistent Fever Diagnosed by Examining the “Forgotten Organ”. JMA J. 2021;4(2):171-173.
Key words: primary splenic lymphoma, forgotten organ, spleen, splenomegaly, multiple splenic hypodense foci, contrast-enhanced computed tomography, fever
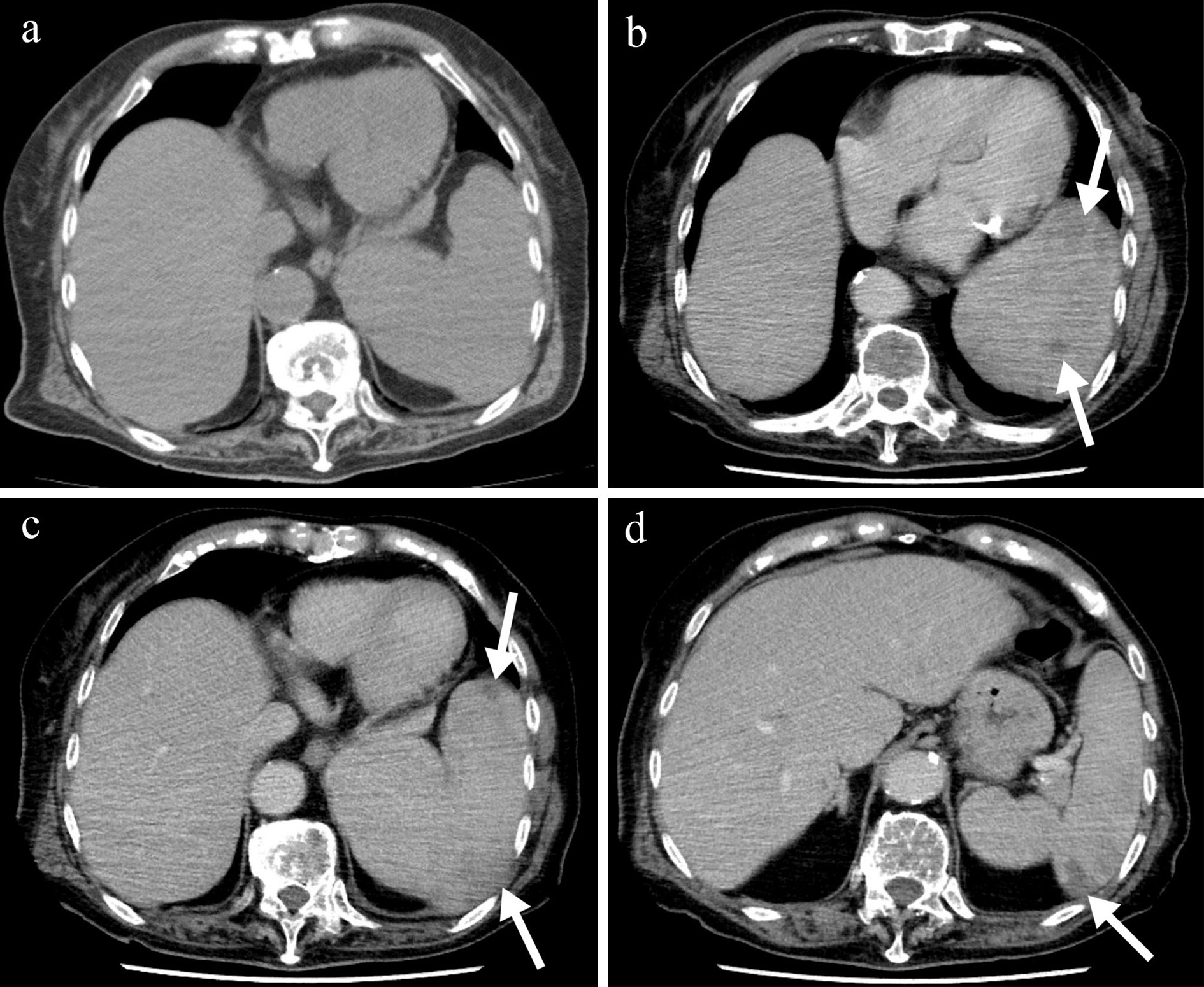
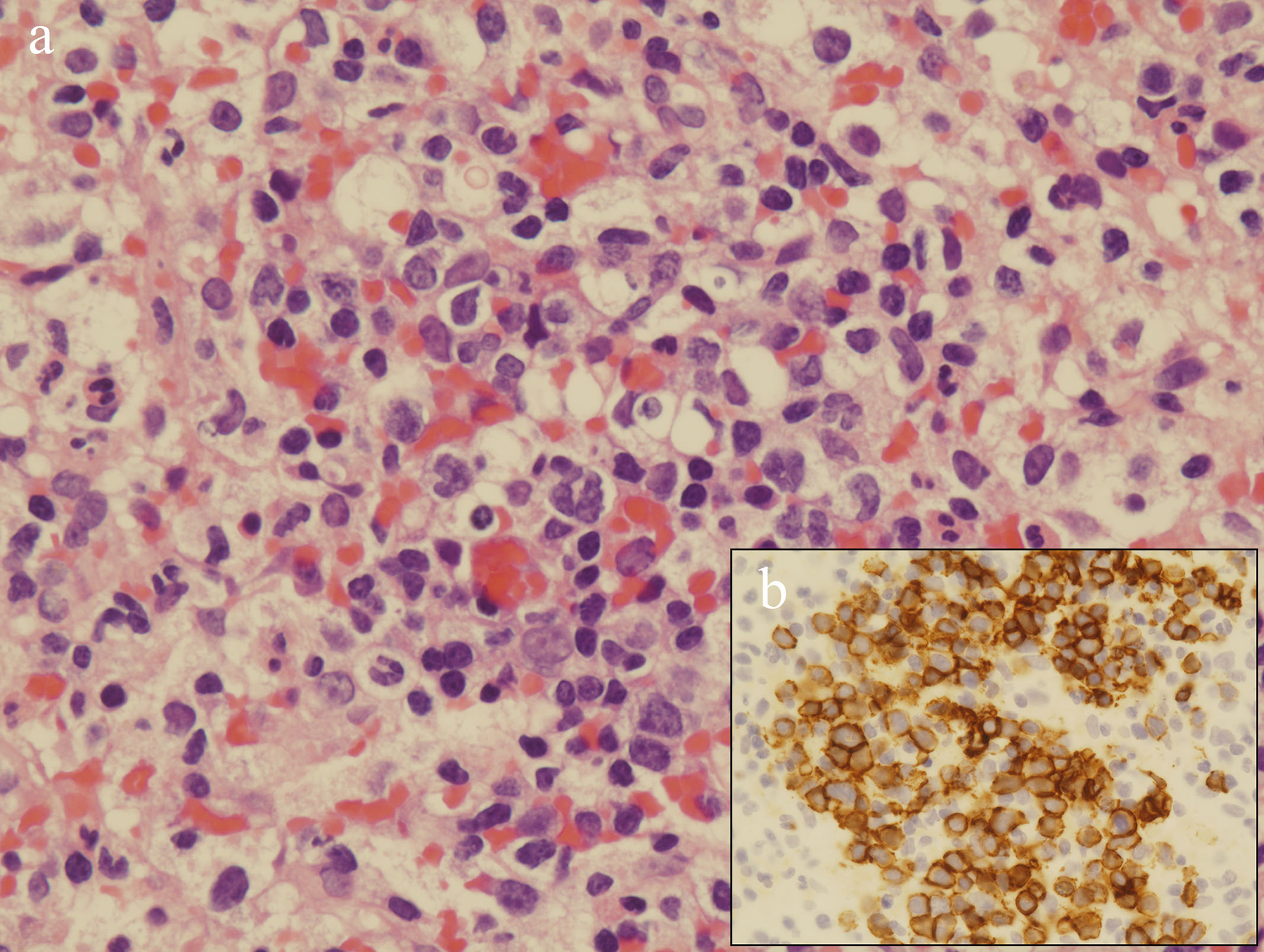
An 88-year-old woman was hospitalized with a 1-day history of fever. Laboratory test results demonstrated a platelet count of 6.3 × 109/L and a lactate dehydrogenase level of 314 U/L. Abdominal ultrasound showed gallstones. Although initially cholecystitis was suspected and cefmetazole was administered, the fever lasted for 1 week. Contrast-enhanced computed tomography (CECT) revealed enlarged spleen, multiple ill-defined splenic hypodense foci, and no lymphadenopathy (Figure 1). Considering the CECT findings (i.e., splenomegaly and multiple splenic hypodense foci with ill-defined margins), the differential diagnosis included primary splenic lymphoma (PSL) or sarcoidosis (1). An ultrasound-guided splenic core needle biopsy was performed, which led to the diagnosis of diffuse large B-cell lymphoma (Figure 2). Subsequently, the patient was transferred to another hospital for treatment.
The spleen is frequently recognized as the “forgotten organ” among clinicians (2). However, splenic imaging studies may help establish the diagnosis. In particular, if a patient presents with persistent fever and splenomegaly, both of which are common symptoms in daily practice, clinicians should keep a high index of suspicion of PSL and perform CECT (3). To arrive at the correct histopathological diagnosis, although splenectomy has generally been performed, splenic biopsy can nowadays be used as an effective diagnostic method with low complication rates (4).
None
HF acquired data and drafted the manuscript. AK, KW, and MS reviewed and supervised the manuscript.
We have obtained informed consent for this manuscript.
In this study, IRB approval was not required.
Karlo CA, Stolzmann P, Do RK, et al. Computed tomography of the spleen: how to interpret the hypodense lesion. Insights Imaging. 2013;4(1):65-76.
Ahmed S, Horton KM, Fishman EK. Splenic incidentalomas. Radiol Clin North Am. 2011;49(2):323-47.
Sun PG, Cheng B, Wang JF, et al. Fever of unknown origin revealed to be primary splenic lymphoma: A rare case report with review of the literature. Mol Clin Oncol. 2017;6(2):177-81.
Ingle SB, Hinge Ingle CR. Primary splenic lymphoma: Current diagnostic trends. World J Clin Cases. 2016;4(12):385-9.
