Corresponding author: Asmita Priyadarshini Khatiwada, asmitapriyadarshinikhatiwada@gmail.com
DOI: 10.31662/jmaj.2021-0015
Received: February 10, 2021
Accepted: April 8, 2022
Advance Publication: September 26, 2022
Published: October 17, 2022
Cite this article as:
Tamang R, Bharati L, Khatiwada AP, Ozaki A, Shrestha S. Pattern of Adverse Drug Reactions Associated with the Use of Anticancer Drugs in an Oncology-Based Hospital of Nepal. JMA J. 2022;5(4):416-426.
Introduction: Adverse drug reactions (ADRs) are among the leading causes of morbidity and mortality worldwide. ADRs of anticancer drugs are ubiquitous. However, in Nepal, studies on chemotherapy-induced ADRs are scarce. Thus, this study aimed to assess the ADRs associated with the use of anticancer drugs and their management along with causality assessment and severity of ADRs.
Methods: A prospective cross-sectional observational and single-center study was conducted at Bhaktapur Cancer Hospital, Nepal, for 6 months. All the patients who fulfilled the study criteria were analyzed to identify ADRs occurring daily. In addition, all collected data were recorded and analyzed using descriptive statistics.
Results: A total of 861 ADRs were detected among 102 cancer patients. The mean ± S.D. age of the patients was 49.93 ± 14.27 years, and each enrolled patient experienced one or more ADRs with a mean ± S.D. of 8.44 ± 3.27. The common ADRs observed were fatigue, anorexia, alopecia, constipation, nausea, vomiting, and neuropathy. Cyclophosphamide, either alone or in combination with other chemotherapeutic agents, was responsible for most ADRs. According to Naranjo’s causality assessment algorithm, most of the ADRs belonged to the probable (47.1%) category. Majority (54.9%) of the ADRs were moderate in their severity. Proton pump inhibitors, antiemetic, mouth gargle, protein powders, iron tablets, and multivitamin and mineral tablets were commonly used for ADR management.
Conclusions: The occurrence of chemotherapy-related ADRs in each enrolled patient is a crucial concern. The present study highlights the need for active monitoring of the patients to identify and manage ADRs promptly.
Key words: Adverse drug event, Adverse drug reaction, Anticancer drugs, Chemotherapy, Nepal
Cancer is one of the most threatening diseases for humans. In 2012, an estimated 14.1 million new cancer cases and 8.2 million cancer-related deaths were observed, and the incidence of cancer is predicted to increase to 19.3 million by 2025 (1). There are different treatment approaches for cancer, such as surgery, chemotherapy, radiation therapy, immunotherapy, and monoclonal antibody therapy, with chemotherapy being commonly used as part of a multimodal treatment strategy for different cancer types (2).
A variety of antineoplastic or chemotherapeutic agents are used to treat cancer and are proven to be beneficial and considerably improve patients’ quality of life. However, the toxicity and narrow therapeutic index of these drugs (3) may extend their therapeutic effects, which can be acute or chronic, temporary or permanent, and mild or potentially life-threatening (4), (5). This makes the vigilance of drug use crucial in every cancer patient.
Adverse drug reaction (ADR) is the fifth leading cause of mortality worldwide, and it accounts for approximately 3%-4% of all hospital admissions (6), (7). Among various drugs associated with ADRs, antineoplastic agents rank first in terms of toxicity (8). Furthermore, the ADRs of anticancer drugs are intensified by the frequent use of a combination of drugs compared with single-drug therapy (9). ADRs associated with antineoplastic agents include alopecia, nausea and vomiting, myelosuppression, cardiac toxicity, hemorrhagic cystitis, mucositis, hot flushes, electrolyte imbalance, and deep vein thrombosis (10). Failure to manage these effects promptly may result in fatal outcomes, increase the healthcare cost for patients, and affect the patients’ quality of life. Hence, timely management of such serious adverse effects is crucial.
Furthermore, studies addressing the ADRs associated with chemotherapy should make the community aware of the potential ADRs. In Nepal, the burden of cancer has been increasing over time, which has increased the need for chemotherapy (11). In 2017, cancer accounted for 10% of the total deaths, and the estimates have been increasingly coming to 2020 (12), (13), with lung cancer being the leading cause of deaths among cancer cases. In addition to lung cancer, cervical, breast, stomach, and colorectal cancers are commonly observed in Nepalese (14). A study using a population-based cancer registry demonstrated that 95.7 per 1000000 population is the age-adjusted incidence rate (15). Although cancer is one of the common diseases observed in Nepal, studies (16), (17), (18), (19), (20), (21) on the ADRs of chemotherapy in oncology-based settings in Nepal are scarce. Likewise, the pharmacovigilance system of anticancer drugs is limited and underreported (22). This may be due to a lack of support from hospital management, lack of team spirit in the admission and reporting of ADRs by the healthcare professionals, and sometimes even the fear of legal implications from patients or the patients’ party (23), (24), (25), (26). Consequently, the current study was conducted to investigate the ADRs of chemotherapeutic agents in general. This study aimed to identify the pattern, frequency, causality, and severity of ADRs experienced by cancer patients taking various chemotherapeutic agents for their relevant conditions as well as to assess the management approaches for the ADRs that occurred.
A prospective cross-sectional observational study was conducted over 6 months from August 2018 to February 2019 at Bhaktapur Cancer Hospital, Bhaktapur, Nepal. It is a 110-bed national-level cancer hospital in Nepal that provides chemotherapy, radiotherapy, surgery, and brachytherapy, including palliative care.
A total of 102 cancer patients were enrolled in this study. The non-probability sampling method (purposive sampling) was employed to determine the sample of the study population. Patients above 18 years old diagnosed with cancer and were on active treatment with chemotherapy were included in this study. Pregnant women and patients being treated with radiotherapy were excluded from this study.
The study was approved by the Institutional Review Board of the Institute of Medicine, Tribhuvan University Teaching Hospital, Kathmandu, Nepal. The permission to conduct the study was given by Bhaktapur Cancer Hospital, Bhaktapur, Nepal. The patients who fulfilled the study criteria were enrolled after written and verbal informed consent was obtained from them and/or their caregivers.
The clinical and demographic data of the participants relevant for the study were obtained from their medical records and documented in the suitably designed data collection form (Annexure 1). All the required details of the suspected ADRs were collected and documented in the same form. The causality of the ADRs was evaluated using Naranjo’s algorithm (27), and severity was assessed using the Modified Hartwig and Siegel scale (28).
Descriptive statistics such as percentage, mean, and standard deviations were used to describe the study variables. The analysis was conducted using the SPSS software for Windows, version 21.0 (IBM Corp., Armonk, NY).
A total of 102 patients who fulfilled the inclusion criteria were enrolled in this study. The patients’ average age was 49.93 ± 14.3 years, and majority (n = 45, 44.1%) of them belonged to the age group of 45-59 years. The ADR distribution was higher in women (n = 74, 72.5%). Majority (n = 28, 27.5%) of the enrolled patients were found to have stage II cancer, and most of them (n = 28, 27.5%) were undergoing the third cycle of chemotherapy. Furthermore, a total of 24 different cancer types were detected in the study, with breast cancer having the highest frequency (n = 35, 34.3%). The detailed demographic, disease, and clinical characteristics of the patients are presented in Table 1.
Table 1. Demographic and Clinical Characteristics of the Study Population.
| Characteristics | Group | Frequency (%) N = 102 |
|---|---|---|
| Age: Mean ± SD | 49.93 ± 14.27 | |
| Age group (years) | 15-29 | 10 (9.8) |
| 30-44 | 18 (17.6) | |
| 45-59 | 45 (44.1) | |
| 60-74 | 25 (24.5) | |
| >75 | 4 (3.9) | |
| Sex | Female | 74 (72.5) |
| Male | 28 (27.5) | |
| Occupation | Farmer | 39 (38.2) |
| Housewife | 31 (30.4) | |
| Business | 12 (11.8) | |
| Student | 5 (4.9) | |
| Service | 9 (8.8) | |
| Others | 6 (5.9) | |
| Marital status | Single | 93 (91.2) |
| Married | 7 (6.9) | |
| Divorced | 2 (2) | |
| Cancer type | Breast cancer | 35 (34.3) |
| Lung cancer | 15(14.7) | |
| Ovarian cancer | 8 (7.8) | |
| Stomach cancer | 6 (5.9) | |
| Rectal cancer | 6 (5.9) | |
| Cervical cancer | 4 (3.9) | |
| Pancreatic Cancer | 3 (2.9) | |
| Immature teratoma | 3 (2.9) | |
| Urinary bladder cancer | 3 (2.9) | |
| Cholangiocarcinoma | 2 (1.9) | |
| Gallbladder Cancer | 2 (1.9) | |
| Choriocarcinoma | 2 (1.9) | |
| Non-Hodgkin lymphoma (NHL) | 2 (1.9) | |
| Colon Cancer | 1 (0.9) | |
| Prostate Cancer | 1 (0.9) | |
| Acute lymphoblastic leukemia (ALL) | 1 (0.9) | |
| Acute myeloid leukemia (AML) | 1 (0.9) | |
| Hodgkin’s Lymphoma | 1 (0.9) | |
| Vulval Cancer | 1 (0.9) | |
| Oesophageal cancer | 1 (0.9) | |
| Gestational Trophoblastic Neoplasia (GTN) | 1 (0.9) | |
| Periampullary cancer | 1 (0.9) | |
| Rectosigmoid cancer | 1 (0.9) | |
| Endometrial cancer | 1 (0.9) | |
| Stage of cancer | I | 7 (6.9) |
| II | 28 (27.5) | |
| III | 25 (24.5) | |
| IV | 25 (24.5) | |
| Stage not defined | 17 (16.6) | |
| Chemotherapy cycle | Second | 19 (18.6) |
| Third | 28 (27.5) | |
| Fourth | 14 (13.7) | |
| Fifth | 20 (19.6) | |
| Sixth | 12 (11.8) | |
| Seventh | 3 (2.9) | |
| Ninth | 4 (3.9) | |
| Others | 2 (2) |
Of the 233 anticancer drugs prescribed for 102 patients in the study, alkylating agents were most frequently prescribed (n = 114, 48.92%). Cyclophosphamide (n = 39, 16.7%), followed by carboplatin (n = 34, 14.6%) and then cisplatin (n = 34, 14.6%), was found to be the widely used alkylating agent. Other classes of anticancer drugs prescribed are listed in Supplementary Table 1.
ADRs were observed in all patients enrolled in the current study, and the mean of the ADRs that occurred was 8.44 ± 3.3. Thus, a total of 861 ADRs were detected in the study. Patients with breast cancer (n = 304, 35.3%) had the highest frequency of ADRs, followed by those with lung cancer (n = 100, 11.6%) and then those with ovarian cancer (n = 65, 7.5%) (Table 2).
Table 2. Types of Cancer and ADR Distribution According to Cancer Type.
| Cancer type | ADR frequency (%) (N=861) |
|---|---|
| Breast cancer | 304 (35.3) |
| Lung cancer | 100 (11.6) |
| Ovarian cancer | 65 (7.5) |
| Stomach cancer | 52 (6.0) |
| Rectal cancer | 51 (5.9) |
| Cervical cancer | 35 (4.0) |
| Pancreatic cancer | 15 (1.7) |
| Urinary bladder cancer | 26 (3.0) |
| Immature teratoma | 26 (3.0) |
| Non-Hodgkin lymphoma (NHL) | 21 (2.4) |
| Cholangiocarcinoma | 22 (2.5) |
| Others* | 144 (16.8) |
| *Others include prostate cancer, esophagus, vulva, GTN, peri ampulla, endometrium, cholangiocarcinoma, and colon. | |
Among 102 patients included in this study, 861 ADRs were recorded, with the most common being fatigue (n = 86, 84.3%), followed by anorexia (n = 81, 79.4%) and alopecia (n = 65, 63.7%). The common hematological reactions were anemia (40.2%) and neutropenia (41.1%). Other adverse reactions are listed in Table 3.
Table 3. Pattern of ADRs Observed.
| Pattern of Adverse drug reactions | Frequency (%) (N=102) |
|---|---|
| Fatigue | 86 (84.3) |
| Anorexia | 81 (79.4) |
| Alopecia | 65 (63.7) |
| Constipation | 44 (43.1) |
| Nausea | 43 (42.1) |
| Neutropenia | 42 (41.1) |
| Anemia | 41 (40.2) |
| Vomiting | 40 (39.2) |
| Neuropathy | 37 (36.2) |
| Injection site reaction | 32 (31.3) |
| Nail changes | 27 (26.4) |
| Malaise | 26 (25.4) |
| Edema | 23 (22.5) |
| Taste changes | 14 (13.7) |
| Weight changes | 16 (15.6) |
| Diarrhea | 17 (16.6) |
| Fever | 19 (18.6) |
| Hyperpigmentation | 14 (13.7) |
| Dyspepsia | 13 (12.7) |
| Febrile neutropenia | 10 (9.8) |
| Blood pressure changes | 9 (8.8) |
| Burning micturition | 9 (8.8) |
| Dyspnea | 9 (8.8) |
| Thrombocytopenia | 8 (7.8) |
| Irregular menses | 7 (6.8) |
| Joint pain | 7 (6.8) |
| Insomnia | 7 (6.8) |
| Anaphylaxis | 5 (4.9) |
| Difficulty swallowing | 5 (4.9) |
| Infection | 6 (5.8) |
| Irritability | 5 (4.9) |
| Flatulence | 5 (4.9) |
| Cough | 4 (3.9) |
| Eye problems | 2 (1.9) |
ADRs of adjuvant chemotherapy (n = 62, 60.8%) were frequently observed, followed by those of palliative care (n = 27, 26.5%) and then curative care (n = 13, 12.7%). Cyclophosphamide was responsible for the occurrence of the majority (n=347, 40.3%) of the ADRs, followed by 5-FU (n=284, 32.9%) and carboplatin (n=266, 30.9%). The list of drugs associated with the observed ADRs is provided in Table 4.
Table 4. Drugs Responsible for Causing ADRs (Alone or in Combination).
| Anticancer drugs | Frequency (%) (N=861) |
|---|---|
| Cyclophosphamide | 347 (40.3) |
| 5-fluorouracil | 284 (32.9) |
| Carboplatin | 266 (30.9) |
| Gemcitabine | 177 (20.5) |
| Docetaxel | 176 (20.4) |
| Doxorubicin | 166 (19.2) |
| Epirubicin | 145 (16.8) |
| Cisplatin | 115 (13.3) |
| Etoposide | 92 (10.6) |
| Paclitaxel | 88 (10.2) |
| Oxaliplatin | 60 (6.9) |
| Vincristine | 54 (6.2) |
| Methotrexate | 53 (6.1) |
| Bleomycin | 44 (5.1) |
| Actinomycin | 36 (4.1) |
| Vinblastine | 18 (2.0) |
| Others | 44 (5.1) |
| *Others: cytarabine, trastuzumab, irinotecan, bicalutamide, pemetrexed, decitabine | |
The most affected organ system was the gastrointestinal (GI) organs (94.1%), followed by the skin (75.4%) and hematological organs (67.6%). Details of the affected system organ class are summarized in Supplementary Table 2.
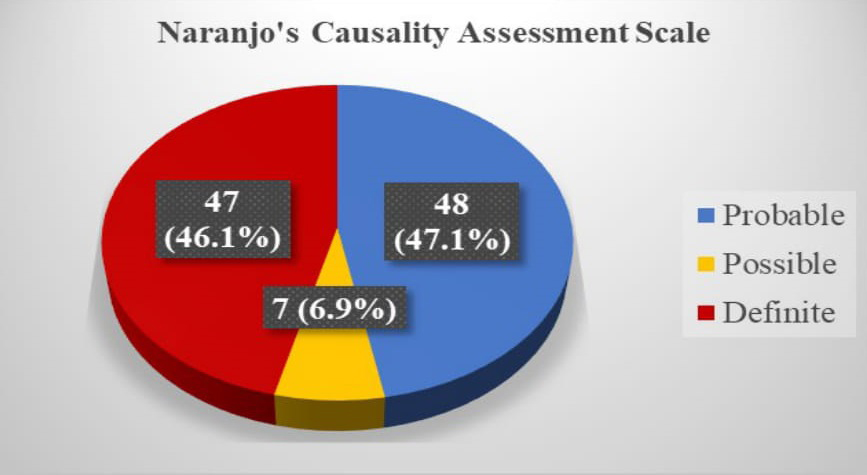
Most of the ADRs belonged to the “probable” category (47.1%), followed by “possible” (46.1%), as assessed using Naranjo’s causality assessment algorithm (Figure 1).
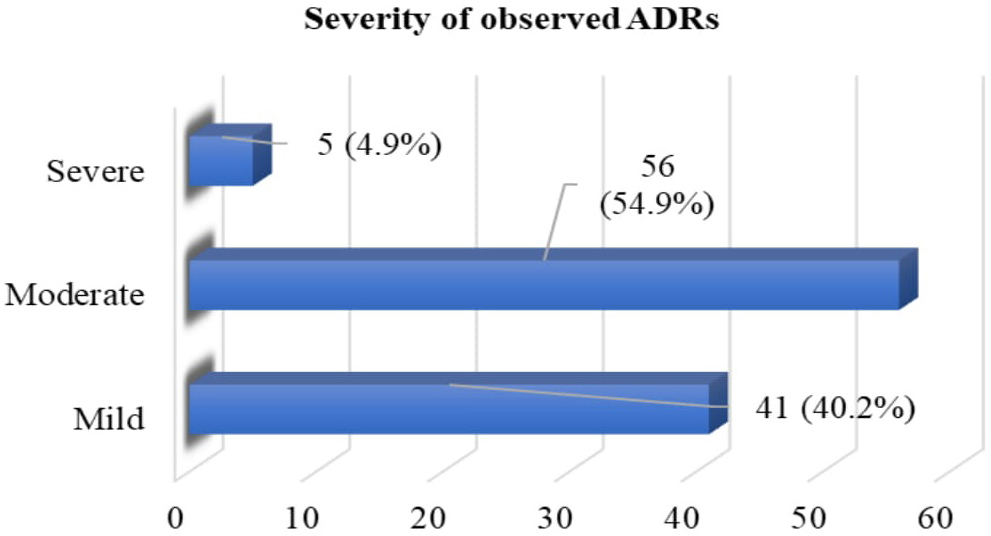
The assessment of the severity of the observed ADRs using the Modified Hartwig and Siegel scale indicated that 54.9% and 40.2% of the ADRs were moderate and mild, respectively (Figure 2).
All the study subjects (n = 102, 100%) were prescribed proton pump inhibitors (PPIs), intravenous (IV) regular saline flush, and antiemetics to manage the ADRs of various chemotherapeutic agents. The different therapeutic classes prescribed to manage the reported ADRs are listed in Table 5.
Table 5. Therapeutic Class Used in ADRs Management.
| Class | Frequency (%) N=102 |
|---|---|
| Proton Pump Inhibitors | 102 (100.0) |
| IV Normal Saline flush | 102 (100.0) |
| Anti-emetics | 102 (100.0) |
| Protein powder | 89 (87.2) |
| Mouth Gargle | 78 (76.4) |
| Iron tablets | 72 (70.5) |
| Inj. Granulocyte colony-stimulating factor | 68 (66.6) |
| Multivitamin mineral tablets | 57 (55.8) |
| Analgesics | 34 (33.3) |
| Antimicrobial agents | 27 (26.4) |
| Laxatives | 25 (24.5) |
| Corticosteroids | 24 (23.5) |
| Appetite stimulant | 23 (22.5) |
| IV mannitol, Potassium Chloride, Magnesium Sulphate | 15 (14.7) |
| Probiotics | 13 (12.7) |
| Folinic acid | 13 (12.7) |
| Pregabalin and Vitamin B-12 | 10 (9.8) |
| Antacid suspension | 7 (6.8) |
| Antispasmodic | 6 (5.8) |
| Antipsychotic | 5 (4.9) |
| Anti-diarrheal agents | 4 (3.9) |
| Antihistamines | 2 (1.9) |
The drugs used to manage various ADRs, such as nausea and vomiting, infections, hematological ADRs, and pain, are presented in Supplementary Table 3.
In the current study, the ADRs of anticancer drugs were observed more in women (n = 74, 72.5%) than in men, a finding consistent with those of other studies conducted in Nepal (17), (19), (20) and its neighboring countries, namely, India (29) and Bangladesh (30). This might be due to the difference in the pharmacokinetic and pharmacodynamic parameters of the drugs between women and men in general, considering the smaller body surface areas of women (31). In addition, the higher number of female patients visiting the hospital during the study period might have led to this result. However, limited studies have demonstrated higher distribution among men (18), (32) and no differences in the distribution between men and women (33).
The mean age of the patients was 49.93 years, with most of the observed ADRs occurring among patients in the age group of 45-59 years (n = 45, 44.4%), a finding similar to those of other few studies (17), (30), (32). The higher incidence of ADRs among older adults may be due to their declining metabolic capacity and excretory function, which leads to the accumulation of the drug in the body resulting in higher adverse outcomes (34).
The study population mainly consisted of farmers (n = 39, 38.2%), followed by housewives (n = 31, 30.4%), and the result was in agreement with that of another study conducted in Nepal (17). Farmers may contact a variety of substances such as pesticides, dust, oils and fumes, microbes, and zoonotic viruses, which are suspected to be carcinogens, making them more prone to cancer (35), (36).
Patients with stage II cancer (n = 28, 27.5%) were frequently observed, and most of them were undergoing the third cycle of chemotherapy. All the patients enrolled in the study experienced ADRs. Overall, the patients in our study experienced ADRs with a mean of 8.44 ± 3.3, whereas in a study conducted by Singh et al., ADRs with a mean of 4.71 ± 2.5 were observed (37). The ADRs may have been induced by the tumor itself and the treatment variables. Polychemotherapy and aging can be considered a few reasons for the increased risk of toxicity. With aging, the bone marrow reserve decreases, which increases the risk of myelosuppression complications caused by chemotherapy (2), (34).
Breast cancer was found to be common among the patients (n = 35, 34.3%), and those with breast cancer (n = 304, 35.3%) had a higher number of ADRs, a finding consistent with those of other studies (29), (30), (38). These findings are interrelated, and the higher number of women in the study supports this result.
Majority of the patients were prescribed alkylating agents, with cyclophosphamide, carboplatin, and cisplatin being the frequently prescribed ones. Cyclophosphamide (n = 347, 40.3%) was mainly responsible for ADR development, whereas other studies demonstrated that cisplatin is the primary drug that induces ADRs (18), (29), (32), (38), (39). Likewise, antimetabolites and alkylating agents were mainly associated with ADRs in a study conducted by Poddar et al (30). Cyclophosphamide is indicated for different malignant conditions, such as Hodgkin’s disease, multiple myeloma, leukemias, breast carcinoma, and adenocarcinoma of the ovary. Some of these conditions were observed in the current study, with breast cancer being the most frequently observed, thus making cyclophosphamide the most prescribed chemotherapeutic agent (40).
In the current study, the most common ADR of anticancer drugs was fatigue, followed by anorexia and alopecia. On the contrary, Poddar et al. reported nausea and vomiting as the common ADRs (30). In other studies, neutropenia and constipation were the commonly observed ADRs (18), (41). Fatigue, a common side effect of chemotherapy, might have resulted from anemia or might have been the outcome of more energy utilization by the body to combat the effects of drugs, the building of new cells, or the disposing of dead cells. Also, factors like poor appetite, emotional stress, pain, and lack of sufficient rest might have led to the condition (42).
Among the system organ classes involved, the GI system (n = 96, 94.1%) was affected mainly by ADRs, a finding similar to those of other studies (29), (38), (43). However, other studies conducted in Nepal demonstrated that the hematological system was mainly affected by the GI system (18), (44). In a single-center study, cyclophosphamide is more associated with GI side effects (45). In the current study, the higher number of cyclophosphamide prescription might have led to more GI side effects.
In this study, an assessment of the causality of ADRs using Naranjo’s algorithm indicated that the majority (n = 48, 47.1%) of the ADRs belonged to the “probable” category, followed by the “definite” category (n = 47, 46.1%), a finding that was in contrast to the results of Chopra et al.’s studies, in which most of the ADRs were under the possible (80%) or probable (20%) category (38). Most of the reactions in the current study were moderate (54.9%), followed by mild (40.2%), a finding that contrasts those of Gunaseelan et al., who reported 74.1% of the ADRs as moderate, followed by 17.9% as mild (46). Furthermore, in a study by Sharma et al., most reactions were mild to moderate and did not require withdrawal or a change in drug therapy (47).
PPIs, IV normal saline flush, and antiemetics were prescribed to all the patients in the current study. The prescription of PPIs for all patients can be justified by the high number of ADRs affecting the GI system. Because patients with cancer are prescribed multiple medications, PPIs are often used as preventive medications for possible gastritis and GI disturbances. However, the use of PPIs needs to be limited to necessary conditions because PPIs interact with and may affect the safety and efficacy of anticancer agents, such as methotrexate, capecitabine, palbociclib, enzalutamide, and anastrozole (48). Also, long-term use of PPIs increases the risk of clostridium difficile and other enteric infections, community-acquired pneumonia, and nutritional deficiencies (49). For every patient undergoing chemotherapy, antiemetics are compulsorily prescribed as prophylaxis; patients who experience nausea or vomiting after or during therapy need to use antiemetics. In addition, IV saline can be given to patients as supportive therapy for diarrhea, dehydration, fatigue, anorexia, and hypotension, thus rationalizing the use of IV saline flush in every patient in the study.
All the patients taking cisplatin (n = 15, 14.7%) were treated with IV fluids such as mannitol 20%, injection potassium chloride, injection magnesium sulfate to prevent nephrotoxicity, and parenteral dexamethasone, ranitidine, and granisetron were given to prevent chemotherapy-induced vomiting. For late-stage emesis, an oral antiemetic was given. In a study conducted by Saini et al., granisetron and ondansetron were prescribed to manage nausea with or without vomiting during the chemotherapy cycles (50). Furthermore, drugs like pheniramine maleate and hydrocortisone were used to manage ADRs, such as restlessness, breathlessness, and rash (50).
Considering all these findings, the authors highlight the need for an effective pharmacovigilance system in Nepal due to the absence of adequate data on adverse effects within the country and the genetic diversity of the Nepalese population. Therefore, the pharmacovigilance system in Nepal should be strengthened (51), (52). The authors also stress the urgent need for clinical pharmacy services from the clinical pharmacist for cancer patients, which will help in the monitoring and management of the ADRs, providing drug or disease-related information to cancer patients, preventing drug-drug interactions, and bridging the gap between patients and providers (53), (54), (55), (56).
Because this is a single-center study, the findings may not be generalized, and the results may not reflect the bigger picture. In addition, the patients’ were not followed up due to time constraints, which might have led to a lack of more comprehensive information. Also, in the study, pairwise drug-ADR information was not determined, thus limiting the understanding about drugs that may be responsible for the occurrence of ADRs.
Chemotherapy-related ADRs are common worldwide, most occurring among the elderly, patients with breast cancer, and patients undergoing cyclophosphamide treatment. The high incidence of these ADRs is a matter of concern. The present study highlights the need for active monitoring of the patients to identify and manage ADRs on time to ensure patient safety. Future interventional studies focused on additional data about the risk factors, including a large cohort, may help promptly detect patients at risk for ADRs and effectively manage the condition.
Dr Akihiko Ozaki reports personal fees from MNES Inc. outside the submitted work.
The authors would like to acknowledge Dr. Bal Mukunda Regmi, Head, Department of Pharmacy, Maharajgunj Medical Campus, Institute of Medicine, Maharajgunj, Kathmandu. The authors would also like to thank all the healthcare professionals of in-patient and daycare units of Bhaktapur Cancer Hospital, Bhaktapur and all the patients and patients’ parties who participated in this study.
RT designed the concept and design acquisition of data and interpretation of data. LB supervised the study by RT for the thesis, made substantial contributions to conception and design, and took part in revising the manuscript critically for important intellectual content. APK and SS made substantial contributions to conception and design, wrote the manuscript’s first draft, and substantially contributed to data interpretation. AO critically revised the manuscript for important intellectual content. All authors agreed to submit to the current journal, gave final approval of the manuscript, and agreed to be accountable for all aspects of the work.
Research Department, Maharajgunj Medical Campus, Institute of Medicine (IOM), Tribhuvan University, Kathmandu Approval code issued by Institutional Review Board: 195(6-11-E)2/075/076. An approval to conduct the study was obtained from the Institutional Review Board (IRB) of the Institute of Medicine, Tribhuvan University Teaching Hospital (TUTH), Kathmandu, Nepal. The permission to conduct the study was given by Bhaktapur Cancer Hospital, Bhaktapur, Nepal. Both verbal and written informed consent was obtained from all the enrolled patients and/or their caregivers.
Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359-86.
Belachew SA, Erku DA, Mekuria AB, et al. Pattern of chemotherapy-related adverse effects among adult cancer patients treated at Gondar University Referral Hospital, Ethiopia: a cross-sectional study. Drug Healthc Patient Saf. 2016;8:83.
Gandhi TK, Bartel SB, Shulman LN, et al. Medication safety in the ambulatory chemotherapy setting. Cancer. 2005;104(11):2477-83.
Remesh A. Toxicities of anti-cancer drugs and its management. Int J Basic Clin Pharmacol. 2012;1(1):2-12.
Singaraju M, Palaian S, Shankar PR, et al. Safety profile and toxicity amelioration strategies of common adverse effects associated with anticancer medications. J Pharm Res Int. 2020;32(11):18-30.
Baniasadi S, Fahimi F, Shalviri G. Developing an adverse drug reaction reporting system at a teaching hospital. Basic Clin Pharmacol Toxicol. 2008;102(4):408-11.
Giardina C, Cutroneo PM, Mocciaro E, et al. Adverse drug reactions in hospitalized patients: results of the FORWARD (facilitation of reporting in hospital ward) study. Front Pharmacol. 2018;9:350.
Routledge PA, O’mahony M, Woodhouse K. Adverse drug reactions in elderly patients. Br J Clin Pharmacol. 2004;57(2):121-6.
Plenderleith IH. Treating the treatment: toxicity of cancer chemotherapy. Can Fam Physician. 1990;36:1827-30.
Albini A, Donatelli F, Noonan D, et al. Bringing new players into the field: onco-pharmacovigilance in the era of cardio-oncology. Intern Emerg Med. 2012;7(2):99-101.
Saud B, Adhikari S, Awasthi M. Cancer burden in Nepal: a call for action. MOJ Proteom Bioinform. 2018;7(5):278-9.
Shrestha G, Thakur RK, Singh R, et al. Cancer burden in Nepal; 1990-2017: an analysis of the Global Burden of Disease study. PLOS ONE. 2021;16(8):e0255499.
The Global Cancer Observatory [Internet]. IARC: Nepal. 2021 Mar [cited 2021 Apr 3]. Available from: https://gco.iarc.fr/today/data/factsheets/populations/524-nepal-fact-sheets.pdf.
Shrestha G, Neupane P, Lamichhane N, et al. Cancer incidence in Nepal: a three-year trend analysis 2013-2015. Asian Pac J Cancer Care. 2020;5(3):145-50.
Subedi R, Dhimal M, Budukh A, et al. Epidemiologic pattern of cancer in Kathmandu Valley, Nepal: findings of population-based cancer registry, 2018. JCO Glob Onco. 2021;(7):443-52.
Thapaliya K, Shrestha A, Prajapti A, et al. Study of pattern of adverse drug reaction due to cancer chemotherapy and their management in hospitalized patient in BP Koirala Memorial Cancer Hospital. J Chitwan Med Coll. 2014;4(4):24-8.
Shrestha S, Shakya R, Shrestha S, et al. Adverse drug reaction due to cancer chemotherapy and its financial burden in different hospitals of Nepal. Int J Pharmacovigilance. 2017;2(1):1-7.
Mallik S, Palaian S, Ojha P, et al. Pattern of adverse drug reactions due to cancer chemotherapy in a tertiary care teaching hospital in Nepal. Pak J Pharm Sci. 2007;20(3):214-8.
Khanal S, Poudel A, Sharan K, et al. Oncology pharmacy practice in a teaching hospital in Nepal. J Oncol Pharm Pract. 2010;16(2):75-9.
Sah SK, Karn A, Shah A, et al. Incidence and attributes of chemotherapy induced myelotoxicity, anemia and neutropenia in adults with cancer in Nepal: a cross-sectional observational study. J Oncol Pharm Pract. 2019;25(8):1823-30.
Sapkota B, Shrestha R, Chapagai S, et al. Validation of risk of chemotherapy-induced neutropenia: experience from oncology hospital of Nepal. Cancer Manag Res. 2020;12:3751-8.
Shrestha S, Shrestha S, Khanal S. Establishment of the first cancer hospital-based pharmacovigilance center in Nepal. Res Social Adm Pharm. 2018;14(11):1088-9.
Biagi C, Montanaro N, Buccellato E, et al. Underreporting in pharmacovigilance: an intervention for Italian GPs (Emilia-Romagna region). Eur J Clin Pharmacol. 2013;69(2):237-44.
Sewal RK, Saini VK, Medhi B. Forensic pharmacovigilance: newer dimension of pharmacovigilance. J Forensic Leg Med. 2015;34:113-8.
Danekhu K, Shrestha S, Aryal S, et al. Healthcare professionals’ knowledge and perception of adverse drug reaction reporting and pharmacovigilance in a tertiary care teaching hospital of Nepal. Hosp Pharm. 2021;56(3):178-86.
Shrestha S, Sharma S, Bhasima R, et al. Impact of an educational intervention on pharmacovigilance knowledge and attitudes among health professionals in a Nepal cancer hospital. BMC Med Educ. 2020;20(1):179.
Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239-45.
Hartwig SC, Siegel J, Schneider PJ. Preventability and severity assessment in reporting adverse drug reactions. Am J Hosp Pharm. 1992;49(9):2229-32.
Kirthi C, Afzal A, Reddy M, et al. A study on the adverse effects of anti-cancer drugs in an oncology center of a tertiary care hospital. Int J Pharm Pharm Sci. 2014;6(2):580-3.
Poddar S, Sultana R, Sultana R, et al. Pattern of adverse drug reactions due to cancer chemotherapy in tertiary care teaching hospital in Bangladesh. Dhaka Univ J Pharm Sci. 2009;8(1):11-6.
Miller MA. Gender-based differences in the toxicity of pharmaceuticals―the Food and Drug Administration’s perspective. Int J Toxicol. 2001;20(3):149-52.
Sharma PK, Misra AK, Gupta A, et al. A retrospective analysis of reporting of adverse drug reactions to oncology drugs: an experience from a national center of clinical excellence. Indian J Pharmacol. 2018;50(5):273-8.
Jose J, Rao PG. Pattern of adverse drug reactions notified by spontaneous reporting in an Indian tertiary care teaching hospital. Pharmacol Res. 2006;54(3):226-33.
Shrestha S, Shrestha S, Khanal S. Polypharmacy in elderly cancer patients: challenges and the way clinical pharmacists can contribute in resource‐limited settings. Aging Med. 2019;2(1):42-9.
Blair A, Malker H, Cantor KP, et al. Cancer among farmers: a review. Scand J Work Environ Health. 1985;11(6):397-407.
Parent M-É, Désy M, Siemiatycki J. Does exposure to agricultural chemicals increase the risk of prostate cancer among farmers? Mcgill J Med. 2009;12(1):70-7.
Singh S, Dhasmana D, Bisht M, et al. Pattern of adverse drug reactions to anti-cancer drugs: a quantitative and qualitative analysis. Indian J Med Paediatr Oncol Off J Indian Soc Med Paediatr Oncol. 2017;38(2):140-5.
Chopra D, Rehan HS, Sharma V, et al. Chemotherapy-induced adverse drug reactions in oncology patients: a prospective observational survey. Indian J Med Paediatr Oncol. 2016;37(1):42-6.
Amartya D. Monitoring of suspected adverse drug reactions in oncology unit of an urban multispeciality teaching hospital. Int J Res Pharm Biomed Sci. 2010;1(2):1-32.
IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Pharmaceuticals. Lyon (France): International Agency for Research on Cancer; 2012. METHYL-CCNU.
Lau PM, Stewart K, Dooley M. The ten most common adverse drug reactions (ADRs) in oncology patients: do they matter to you? Support Care Cancer. 2004;12(9):626-33.
Madeddu C, Gramignano G, Astara G, et al. Pathogenesis and treatment options of cancer related anemia: perspective for a targeted mechanism-based approach. Front Physiol. 2018;9:1294.
Guo H-j, Ren F, Zhang D, et al. Monitoring report on 341 cases of adverse reactions caused by antitumor drugs. Afr J Microbiol Res. 2012;6(16):3774-7.
Behera SK, Kishtapati CR, Gunaseelan V, et al. Chemotherapy induced adverse drug reactions in cancer patients in a tertiary care hospital in South India. J Young Pharm. 2017;9(4):593-7.
Dan DC, Fischer R, Adler S, et al. Cyclophosphamide: as bad as its reputation? Long-term single centre experience of cyclophosphamide side effects in the treatment of systemic autoimmune diseases. Swiss Med Wkly. 2014;144:w14030.
Gunaseelan V, Mandal SK, Prasad V, et al. Adverse drug reactions to cancer chemotherapy in a regional cancer center in Northeast India. Int J Pharm Sci Res. 2014;5(8):3358.
Sharma A, Kumari KM, Manohar HD, et al. Pattern of adverse drug reactions due to cancer chemotherapy in a tertiary care hospital in South India. Perspect Clin Res. 2015;6(2):109-15.
Uchiyama AAT, Silva PAIA, Lopes MSM, et al. Proton pump inhibitors and oncologic treatment efficacy: a practical review of the literature for oncologists. Curr Oncol. 2021;28(1):783-99.
Triadafilopoulos G, Roorda AK, Akiyama J. Indications and safety of proton pump inhibitor drug use in patients with cancer. Expert Opin Drug Saf. 2013;12(5):659-72.
Saini V, Sewal R, Ahmad Y, et al. Prospective observational study of adverse drug reactions of anti-cancer drugs used in cancer treatment in a tertiary care hospital. Indian J Pharm Sci. 2015;77(6):687-93.
Shrestha S, Danekhu K, KC B, et al. Bibliometric analysis of adverse drug reactions and pharmacovigilance research activities in Nepal. Ther Adv Drug Saf. 2020;11:2042098620922480.
Sharma S, Khanal T, Shrestha S, et al. A celebration of World Pharmacist Day 2018 focusing to strengthen the pharmacy services at an oncology-based hospital in Nepal: iInspiration for others in developing countries. Res Social Adm Pharm. 2019;15(1):117-8.
Shrestha S, Shakya S, Khatiwada AP. An Urgent Necessityurgent necessity for Clinical Pharmacy Servicesclinical pharmacy services in Cancer Carecancer care in Nepal. JCO Glob Oncol. 2020;6:1392-3.
Shrestha S, Shakya D, Palaian S. Clinical pharmacy education and practice in Nepal: a glimpse into present challenges and potential solutions. Adv Med Educ Pract. 2020;11:541-8.
Shrestha S, Shrestha S, Palaian S. Can clinical pharmacists bridge a gap between medical oncologists and patients in resource-limited oncology settings? An experience in Nepal. J Oncol Pharm Pract. 2018;25(3):765-8.
Shrestha S, Khatiwada AP, Gyawali S, et al. Overview, challenges and future prospects of drug information services in Nepal: a reflective commentary. J Multidiscip Healthc. 2020;13:287-95.