Corresponding author: Naoya Fujita, raoh0615@gmail.com
DOI: 10.31662/jmaj.2023-0063
Received: April 19, 2023
Accepted: June 6, 2023
Advance Publication: September 13, 2023
Published: October 16, 2023
Cite this article as:
Fujita N, Ono Y. Wandering Pneumonia. JMA J. 2023;6(4):543-545.
Key words: Wandering pneumonia, IgG4-related lung disease, IgG4-related disease
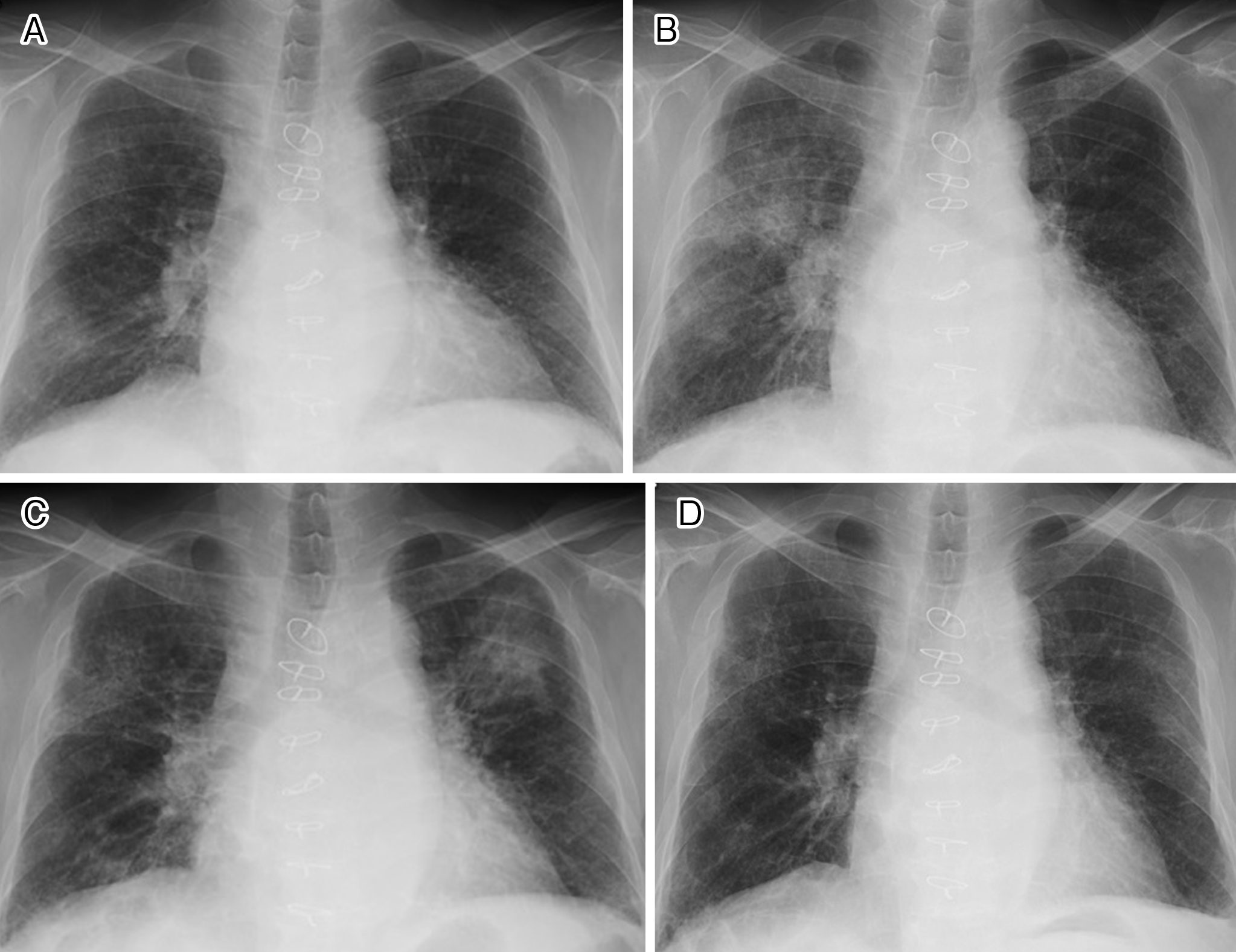
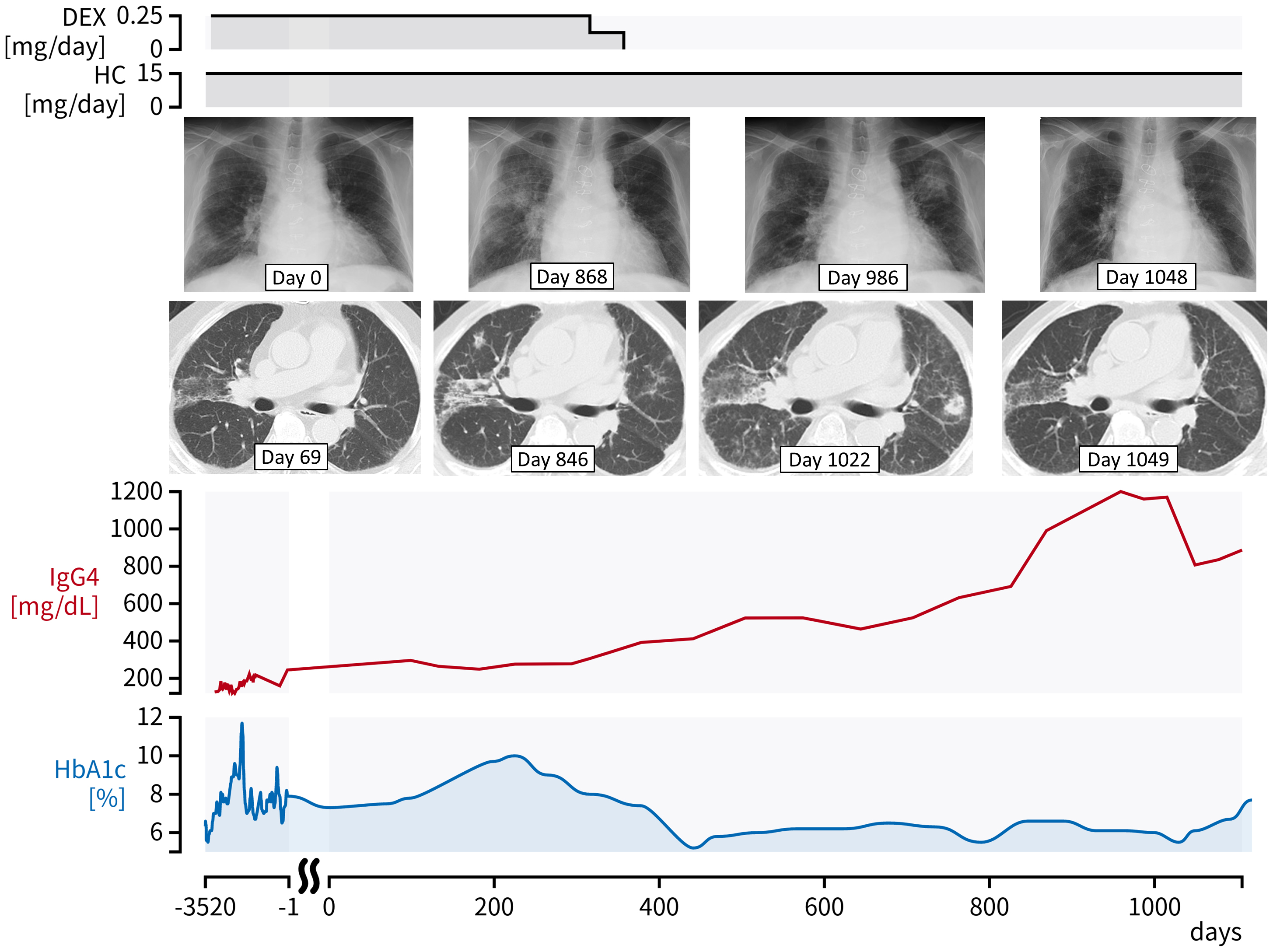
A 74-year-old man was referred for chest X-ray abnormalities (Figure 1a). He had a history of hypopituitarism with pituitary stalk enlargement, soft tissues around the infrarenal and iliac arteries, and elevated serum IgG4 levels (150-250 mg/dL; reference range, 11-121 mg/dL), suggesting IgG4-related disease (1). He was treated with oral hydrocortisone and dexamethasone for hypopituitarism. Fine crackles were heard on chest auscultation. Computed tomography showed pulmonary ground-glass opacities with peribronchovascular and septal thickening. Because he was asymptomatic, he refused further investigation and underwent follow-up only. Dexamethasone was tapered and discontinued because of the exacerbation of diabetes mellitus, whereas the lung lesions progressed and the serum IgG4 levels increased. Subsequent chest X-rays at 868, 986, and 1,048 days after the first X-ray revealed spontaneous migration or disappearance of the shadows (Figure 1b-d), consistent with so-called “wandering pneumonia” (2). His serum IgG4 levels increased to 800-1,200 mg/dL during this time (Figure 2), but he had no respiratory manifestations even without immunosuppressive therapy. Thus, the imaging changes may have shown the formation of IgG4-related lung disease (IgG4RLD) over time (3). Although the long-term course of IgG4RLD is unclear, the present findings may be a feature of IgG4RLD.
None
This work was supported by the Japan Medical Education Foundation (https://www.jmef.or.jp/). The funders played no role in the preparation of the manuscript or the decision to publish.
NF wrote the first draft of the manuscript and contributed to patient care. YO revised and organized the manuscript.
The patient provided written informed consent for the publication of the manuscript and the clinical images.
This study did not require IRB approval.
Wallace ZS, Naden RP, Chari S, et al. The 2019 American College of Rheumatology/European League against rheumatism classification criteria for IgG4-related disease. Arthritis Rheumatol. 2020;72(1):7-19.
Yoshida Y, Saraya T, Fujiwara M, et al. Wandering pneumonia mimicked by COVID-19. Intern Med. 2021;60(3):493-4.
Yamasue M, Kushima H, Ishii H, et al. A case of IgG4-related lung disease presenting with wandering shadows. Nihon Kokyuki Gakkaishi. 2014;3(5):719-22.
