Corresponding author: Naohiro Uchio, n-uchio@umin.ac.jp
DOI: 10.31662/jmaj.2024-0425
Received: December 25, 2024
Accepted: February 10, 2025
Advance Publication: March 21, 2025
Published: April 28, 2025
Cite this article as:
Sato R, Uchio N, Takagi H, Matsumoto H. Forearm Magnetic Resonance Imaging Findings in Epidemic Myalgia. JMA J. 2025;8(2):624-626.
Key words: epidemic myalgia, parechovirus A3, STIR hyperintensity
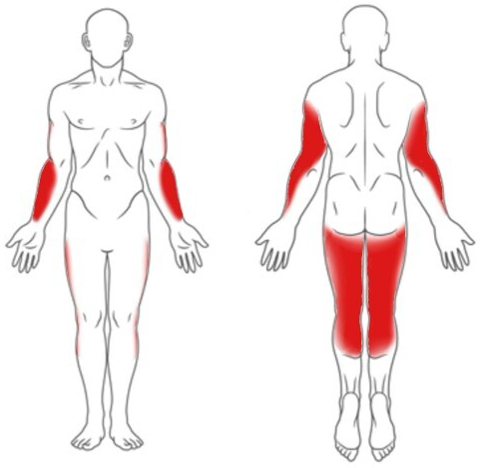
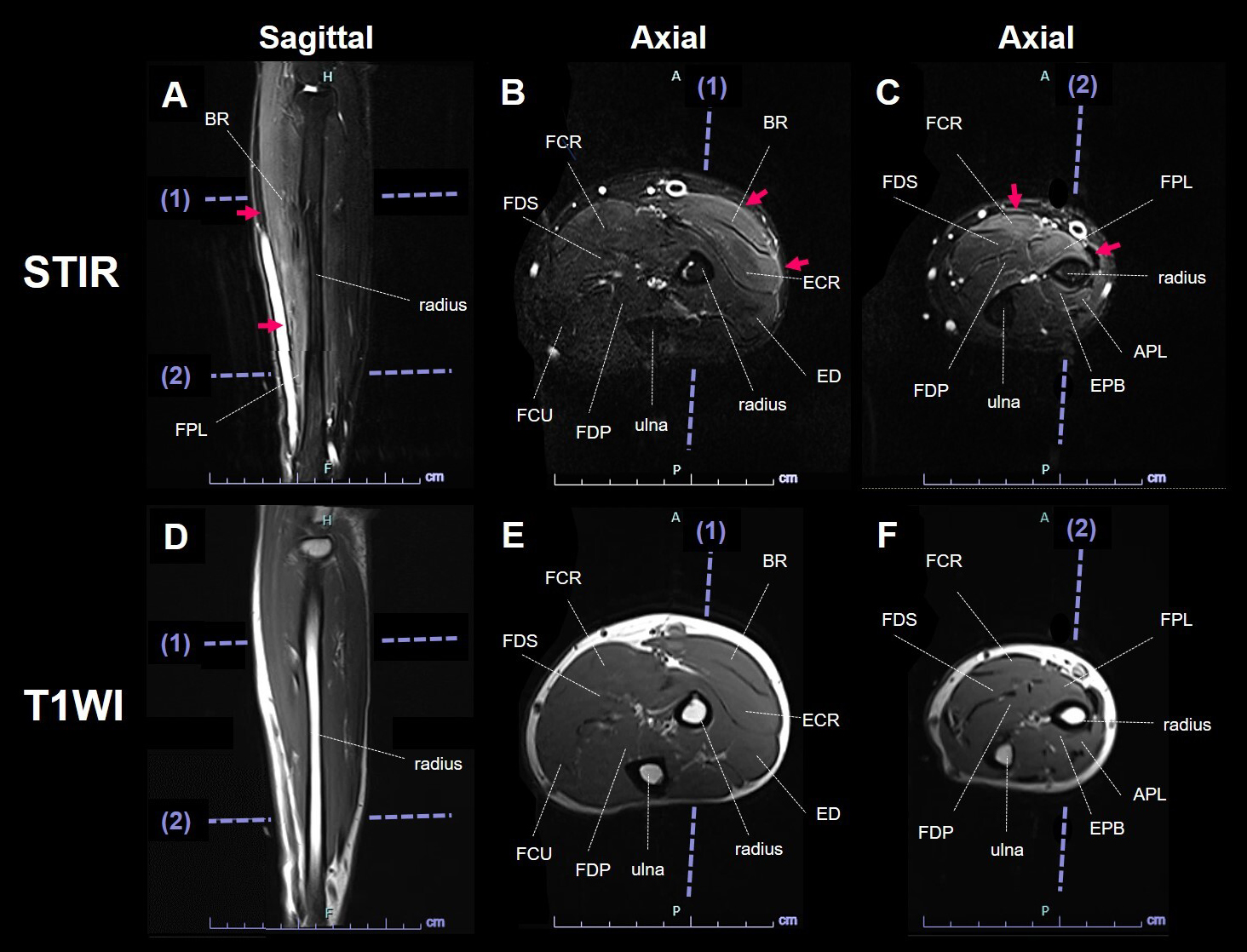
A 34-year-old man presented with myalgia after a fever. Neurological examination revealed myalgia in the posterior upper arms, radial forearms, and posterior lower extremities (Figure 1) and muscle weakness in the distal upper extremities, including the wrist flexor, wrist extensor, flexor digitorum superficialis, and flexor digitorum profundus muscles. Laboratory data showed elevated creatine kinase (1927 IU/L). Magnetic resonance imaging (MRI) indicated short-tau inversion recovery (STIR) hyperintensity in the radial forearm muscles and fascia (Figure 2). Epidemic myalgia was diagnosed by detecting parechovirus A3 ribonucleic acid in the patient’s stool. Epidemic myalgia typically shows limb myalgia and decreased grip strength (1). Although STIR hyperintensity in the muscles and fascia in the posterior upper arm and thigh is documented, forearm MRI findings have not been reported (1), (2), (3), (4). The radial forearm STIR hyperintensity aligns with myalgia site rather than muscle weakness. Further studies incorporating forearm findings are needed to clarify the relationship between MRI findings and myalgia.
None
RS, NU, HT, and HM were involved in the acquisition, analysis, or interpretation of data. RS and NU drafted the manuscript. All authors contributed to the revision of the manuscript and approved the final version.
Not applicable.
The patient signed informed consent forms for academic use of the data.
Yamakawa T, Mizuta K, Kurokawa K, et al. Clinical characteristics of 17 adult patients with epidemic myalgia associated with human parechovirus type 3 infection. Rinsho Shinkeigaku. 2017;57(9):485-91.
Shinomoto M, Kawasaki T, Sugahara T, et al. First report of human parechovirus type 3 infection in a pregnant woman. Int J Infect Dis. 2017;59:22-4.
Orimo K, Hatano K, Sato N, et al. Clinical characteristics of epidemic myalgia associated with human parechovirus type 3 during the summer of 2019. Intern Med. 2020;59(14):1721-6.
Masuda S, Koizumi K, Sato M, et al. Severe generalized epidemic myalgia in an adult due to human Parechovirus type 3: a case report. Cureus. 2022;14(10):e30587.