Corresponding author: Takahiro Kobayashi, takakoba3733@gmail.com
DOI: 10.31662/jmaj.2025-0117
Received: March 3, 2025
Accepted: May 2, 2025
Advance Publication: June 20, 2025
Published: July 15, 2025
Cite this article as:
Kobayashi T, Ono Y, Hirooka N. Methotrexate-associated Hodgkin Lymphoma Occurring Decades after Methotrexate Initiation. JMA J. 2025;8(3):998-999.
Key words: methotrexate-associated lymphoproliferative disorder, Hodgkin lymphoma, rheumatoid arthritis
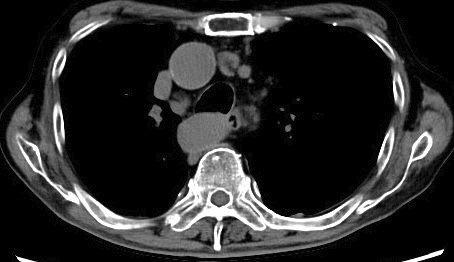
An 84-year-old man with a 40-year history of rheumatoid arthritis (RA), treated with methotrexate (MTX) for decades, presented with an eight-month history of intermittent fever and fatigue. Physical examination revealed lymphadenopathy and RA-associated finger deformities. Laboratory tests showed elevated levels of soluble interleukin-2 receptor (8,452.7 U/mL, reference range: 157-474) and C-reactive protein (11.7 mg/dL), as well as a decreased lymphocyte count. Chest computed tomography revealed multiple enlarged lymph nodes in the axillary, peritoneal, para-aortic, and mediastinal regions (Figure 1). MTX was immediately discontinued, and a subsequent pathological investigation of an inguinal lymph node showed large malignant lymphocytes with positive Epstein-Barr virus (EBV)-encoded small ribonucleic acid and Reed-Sternberg cells, indicating a diagnosis of stage Ⅲ mixed cellularity classic Hodgkin lymphoma. The patient’s EBV-related antibody status was: anti-viral capsid antigen (VCA) immunoglobulin (Ig)M (-), VCA IgG (+), EBV nuclear antigen IgG (+), suggesting a past EBV infection. Discontinuation of MTX resolved the fever within 1 week and was followed by a reduction in lymph node size over 5 months (Figure 2). This lymphoma is classified as MTX-associated lymphoproliferative disorder (MTX-LPD). According to the revised 4th WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues, MTX-LPD falls under the category of other iatrogenic immunodeficiency-associated lymphoproliferative disorders (1). Hodgkin lymphoma is a common pathological finding seen in MTX-LPD, following diffuse large B-cell lymphoma (2). MTX-LPD can be managed without chemotherapy, as remission can be achieved in 50-60% of the cases by simply eliminating MTX (2), (3). As seen in this case, EBV plays a substantial role in the pathogenesis of MTX-LPD, even in the latent phase following a prior infection (4). There is growing awareness of MTX-LPD because of its Asian-dominant prevalence (2), and MTX-LPD should be considered regardless of the size and distribution of lymphadenopathy, or the duration of MTX administration, even for decades, as in this case. Furthermore, the prompt discontinuation of MTX prior to pathologic diagnosis, as was implemented in this case, is crucial for rapid diagnosis without overlooking self-limiting conditions.
None
Takahiro Kobayashi wrote the first draft of the manuscript. Yosuke Ono and Nobutaka Hirooka revised the manuscript. Takahiro Kobayashi, Yosuke Ono, and Nobutaka Hirooka contributed to the patient care. Takahiro Kobayashi organized the manuscript.
Not applicable.
The written consent form was obtained from the patient about publishing manuscripts and photographs.
Swerdlow SH, Campo E, Harris NL, et al. Other iatrogenic immunodeficiency associated lymphoproliferative disorders. In: Swerdlow SH, Campo E, Harris NL, et al., editors. WHO classification of tumors of the haematopoietic and lymphoid tissues. 4th ed. Vol. 2. Lyon, France: International Agency for Research on Cancer; 2017. p. 462-4.
Kuramoto N, Saito S, Fujii T, et al. Characteristics of rheumatoid arthritis with immunodeficiency-associated lymphoproliferative disorders to regress spontaneously by the withdrawal of methotrexate and their clinical course: a retrospective, multicenter, case-control study. Mod Rheumatol. 2022;32(1):24-31.
Yoshihara R, Uefuji A, Muratra M, et al. Clinical manifestations of twenty-seven cases of methotrexate-associated lymphoproliferative disorders. Clin Rheumatol Rel Res. 2017;29:164-72. Japanese.
Miyazaki T, Fujimaki K, Shirasugi Y, et al. Remission of lymphoma after withdrawal of methotrexate in rheumatoid arthritis: relationship with type of latent Epstein-Barr virus infection. Am J Hematol. 2007;82(12):1106-9.